 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 39, No. 3, (July - September 2002), pp. 106-111 A case of carcinoma rete testis: Histomorphological, immunohistochemical and ultrastructural findings and review of literature Palat K. Menon,1 M.D., Ph.D.; Vasudevarao,2 M.D.; Abha Sabhiki,3 M.D.; Sandip Kudesia,4 M.D., Ph.D.; D. P. Joshi,5 M.S., M.C.H.; U. B. Mathur,6 M.D., D.C.P.
1Associate Professor, Department of Microbiology AFMC, Pune
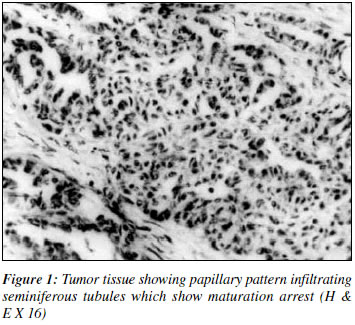
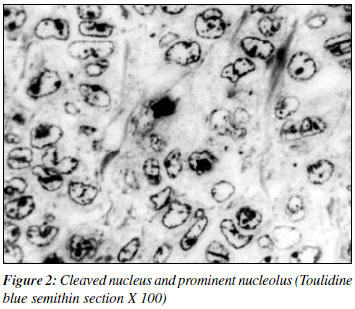
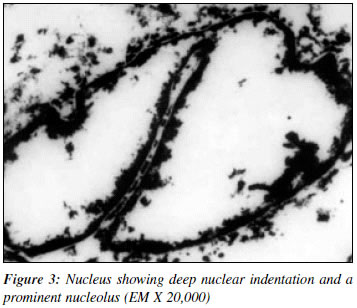
Code Number: cn02004 ABSTRACT A 72-year-old man presenting with a secondary hydrocoel underwent orchidectomy. Gross examination revealed a tumor arising in the region of the rete testis, which on histopathology proved to be a papillary adenocarcinoma. The patient did not have evidence of any other neoplasia elsewhere in the body. The lesion fulfilled the anatomic criteria elucidated by Nochomovitz et al to be labelled as adenocarcinoma of Rete testis. Electron microscopy revealed characteristic nuclear infoldings and microtubules with two different arrangements. The tubules were either seen to form concentric circles or were in irregular groups with filaments interspersed. The lesion on immunohistochemistry was negative for germ cell markers AFP and HCG, and was positive for cytokeratin and epithelial membrane antigen. A review of literature is also presented. INTRODUCTION Adenocarcinoma of the rete testis is a rare tumor with only forty-four human cases reported in world literature.1-44 The light microscopic features are characteristic of papillary adenocarcinoma, however, gross examination is obligatory to identify the site of origin from the rete or mediastinum testis. Diagnostic criteria for adenocarcinoma rete testis as suggested by Nochomovitz23 include, involvement centered around the hilus, lack of direct extension through the tunics, transition from normal to tumor epithelium, no evidence of teratoma and lack of any other primary tumor elsewhere in the body. Only a few cases of ultrastructural studies on adenocarcinoma rete testis have been reported.23,24,27 An experimental model for adenocarcinoma rete testis was developed in mice by in utero exposure to di-ethyl stilbesterol.45-48 We report the clinicopathological features, electron microscopic (EM) and immuno-histochemical findings in a case of adenocarcinoma rete testis occurring in a 72-year-old man. CASE REPORT A 72-year-old man presented with swelling of the left scrotum for a period of two years. The swelling was painless and gradually increasing in size. There was no history of trauma. The swelling was fluctuant but nontranslucent. He was clinically diagnosed to have a secondary hydrocoel. A complete general physical examination did not reveal any abnormality. Per-rectal examination revealed a normal prostate. Xiagram of the chest was normal. Haematological parameters were within normal limits. The patient was taken up for excision and eversion of the sac. At surgery the testis was seen to be covered by multiple small firm nodules. A high inguinal ligation was done and the left testis with sac, vas deferens and epididymis was removed. Postoperative period and recovery was uneventful. Patient was not willing for further therapy and on discharge from hospital did not return for follow up. The specimen was sent for histopathology in formal saline. On gross examination, the specimen consisted of testis surrounded by an open everted collar of the hydrocoel sac measuring 6x6x5 cms. The proximal end showed the vas along with pampiniform plexus. No lymphnodes could be dissected. The tunica vaginalis appeared to be thickened. Transverse section of the mass revealed firm white tumour tissue about 3 cms in diameter arising in the region of the mediastinum testis infiltrating the brownish testicular substance, which was compressed towards the tunica. There were no areas of hemorrhage or necrosis. Representative areas were routinely processed and paraffin sections were stained by hematoxylin eosin, Periodic Acid Schiff (PAS), mucicarmine, Alcian blue, Masons trichrome and silver reticulin. A few bits of tissue were refixed in buffered glutaraldehyde and processed for electron microscopic studies. The semi thin araldite sections were stained with toluidine blue and the ultra thin sections with uranyl acetate and lead citrate. Electron microscopy was done using a Jeol 100 CX electron microscope. Haematoxylin-eosin stained sections showed a tumour arising from the region of the rete testis, infiltrating into the testicular substance. The seminiferous tubules showed maturation arrest (Figure 1). The tumor consisted of small round cells arranged variously in cords, nests and papillary formations. Patchy areas of necrosis were also seen. The neoplastic cells exhibited a high nucleocytoplasmic ratio with a large vescicular nucleus and prominent nucleolus. Mitotic index was about 2-3 per HPF. Transition from normal to neoplastic epithelium was seen in the rete testis. No teratomatous elements were seen. The tumor mass did not penetrate the tunica vaginalis. Abundant stromal connective tissue was seen in the form of thick bundles of vascularised collagen fibers separating groups of cells and acini. The tumor cells were PAS positive and negative for Alcian Blue and Mucicarmine. Toulidine blue semithin sections revealed, the deep indentation of the nuclear membrane almost cleaving the nucleus, margination of the nucleoplasm and prominent nucleolus (Figure 2). On immunohistochemistry the tumor cells were negative for germ cell markers AFP and HCG, and were positive for cytokeratin and epithelial membrane antigen. On electron microscopy the cells were uniformly round to oval and gave a monomorphic picture at lower scanning magnifications. Most of the nuclei showed margination of the nucleoplasm and prominent nucleolus. The nuclear membrane in many cells showed a single deep cleavage, which almost split the nucleus (Figure 3). The cytoplasm showed organelles like rough endoplasmic reticulum, free ribosomes, mitochondria and some had electron dense fat vacuoles. Also seen were cell junctions or desmosomes. In addition the cytoplasm of a few cells had two distinct types of inclusions. The more clearly defined structures were groups of non-membrane bound microtubules of approximately 15 to 45 nm diameter arranged in a concentric manner. These tubules were closely placed but discrete and the intertubular matrix was unremarkable. The other structure that was even less frequent was also not membrane bound but lying adjacent to the nucleus consisted of irregular collection of microtubules of diameter 10 nm. However in these aggregates, fine filaments 13 nm in diameter were haphazardly distributed between the tubules. Both longitudinal and transverse profiles were seen. DISCUSSION Carcinoma rete testis is a rare tumor occurring between 20 to 80 years of age . Of the forty-four cases discussed in literature, three of the ,youngest cases (ages 20 yrs, 21 yrs, and 34 yrs) had a prior history of undescended testis.4,5,20 No particular side was prone to be affected and in one case the tumor was bilateral. No racial preponderance has been evident. In the present case the tumor arose in the left testis of an elderly Indian Male. This is the third case being reported from India.10,12 It presented as a nontender, non translucent hydrocoel gradually increasing in size for which he underwent high inguinal orchidectomy. The tumor was firm to cut and showed white to pale yellow mass. Histopathology showed a papillary adenocarcinoma with areas of microscopic hemorrhage and necrosis. The tumor involvement centered around the region of the rete testis and infiltrated the testicular substance. The transition from normal to tumor epithelium could be demonstrated. There was no evidence of any teratomatous element and the tumor did not penetrate the tunica thus fulfilling all the diagnostic criteria of Nochomovitz et al.23 Malignant mesothelioma is the most important differential diagnosis of adenocarcinoma rete testis. In the present case PAS positive tumor cells which was Alcian blue and Mucicarmine negative supports the diagnosis of adenocarcinoma vis a vis mesothelioma.27 The lesion on immunohistochemistry was negative for germ cell markers AFP and HCG, and was positive for cytokeratin and epithelial membrane antigen. This suggests the epithelial cell origin of the tumor cells. Ultra structural studies in four cases of carcinoma rete testis has been previously reported.22-24,31 Mrak31 used EM to determine the nature of a secondary metastatic lesion in a patient who had previously undergone orchidectomy for carcinoma rete testis. The ultrastructure of normal rete testis has been previously published.22,31,49 Normal rete epithelium is a low columnar ciliated epithelium. Ultrastructurally the nucleus is cleaved, the nucleoplasm is coarse clumped, the nucleoli are rare and marginally located. The cytoplasm though not rich in organelles does show mitochondria, ribosomes, and rough endoplasmic reticulum along with Golgi bodies. Other elements like apical lipid droplets, tonofilaments, basally situated membrane bound vacuoles appear to be more specific to normal rete epithelium. Laterally the cells form pentalaminate desmosomes. In the present case EM studies done on the tumor tissue revealed the deep nuclear indentation a character retained from the normal cells of rete testis. Margination of the nucleoplasm and a single prominent central nucleolus was an additional feature of the tumor cells. This change in nuclear character has also been reported previously.22-24 Microvilli with filamentous cores as described by Crisp-Lindegren27 or those with bulbous ends without filamentous cores as described by Mrak31 were not seen in the present case. Membrane bound granules described by Mrak were also not evident. Desmosomes and electron dense apical lipid droplets were rare. The non-membrane bound tubular inclusions in the cytoplasm of a few cells were comparable to that reported by Fukunaga et al.22 However the second type of structures described by us as a combination of fine tubules and filaments has not been illustrated in any study. The findings though unequivocal do not throw any light to indicate cellular differentiation or its biological behaviour. These inclusions have not been a feature in studies on normal rete testis. Recent molecular studies48 have shown altered regulation of an estrogen responsive gene, lactotransferrin (LTF) in the seminal vesicles of Diethyl stilbestrol treated mice, but not the controls. At the molecular level altered methylation of the gene appears to be involved. The induction of "imprinted" responses during the development of a relatively estrogen-free reproductive tract cell suggests that undifferentiated targets for estrogen action may be sites for subsequent growth and differentiation defects associated with neoplasia. Review of literature suggests that tumor sizes less than 5 cms are less likely to metastasize.37 Retro-peritoneal lymph node dissection and palliative chemotherapy and radiotherapy have been offered to patients with variable results. Our patient however was unwilling for further surgery or radiotherapy and was lost to follow up. REFERENCES
Copyright 2002 - Indian Journal of Cancer. The following images related to this document are available:Photo images[cn02004f3.jpg] [cn02004f1.jpg] [cn02004f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}