 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
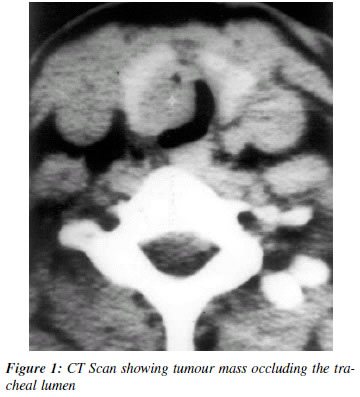
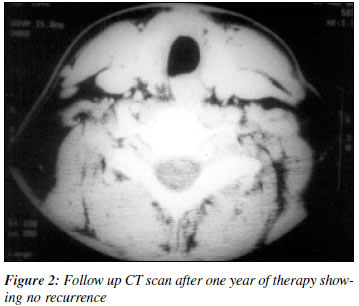
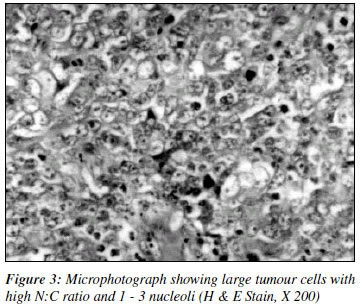
Indian Journal of Cancer, Vol. 39, No. 3, (July - September 2002), pp. 112-115 Tracheal Lymphoepithelioma-like Carcinoma: A Case Report S. Satyanarayana, M.D. (Pathology), S. D. Pathak, M.S. (ENT), V. Saraswat, M.S. (Anaesthesioloy), Y. S. Sarma, M.D. (Medicine) D.M. (Med Oncology), R. Bharadwaj M.D. (Pathology), Y. K. Goorha, M.D. (Pathology) Department of Pathology, Armed Forces Medical College, Departments of ENT and Anaesthesiology, Base Hospital, Delhi Cantt; Department of Pathology, Army Hospital (R&R), Delhi Cantt Code Number: cn02005 ABSTRACT Lymphoepithelioma like carcinoma is rare in locations other than nasopharynx. We report the second case of this tumour in trachea, in a young female patient, who was managed with concomitent surgery, radiotherapy and chemotherapy. The patient is disease free in the one-year follow up. The tumour presented difficulties during intubation for general anaesthesia and during surgery. Association with Epstein-Barr virus was not found in our case. Key Words: Lymphoepithelioma, Poorly differentiated Carcinoma, Trachea. INTRODUCTION Lymphoepitheliomas are malignant tumours of epithelial origin, initially described in the nasopharynx1 are exceedingly rare in other locations with only isolated case reports of occurrence in hypopharynx, uterine cervix,2 skin,3 and breast.4 These tumours are not linked to tobacco or alcohol but have strong association with Epstein-Barr Virus (EBV).5 Usually these tumours present as metastatic disease of un-known primary. Histologically also these tumors form an important lesion in the differential diagnosis of poorly differentiated neoplasms and lymphomas. This tumor presenting as primary lung tumor has been reported.6 Toker et al reported the occurrence in the vocal cords.7 Onizuka M et al reported a case in the trachea.8 We believe that our case is the second case of poorly differentiated lymphoepithelioma- like carcinoma of nasopharyngeal type in the upper trachea in a twenty-six year old female patient. CASE REPORT A 26-year-old lady presented with cough, mucoid expectoration and effortful breathing of three months duration. On quite a few occasions she had expectorated blood tinged sputum and once a dark, reddish, fleshy mass of about 1 cm size following which she had temporary relief of symptoms. A practitioner managed her as a case of bronchial asthma. Her symptoms recurred getting temporary relief only after spitting out of small fleshy masses mixed with blood. At our center, she was found to be in severe respiratory distress with inspiratory stridor. Her general physical examination was normal. There was no pallor, cyanosis, clubbing or any lymphadenopathy. Radiograph of chest was normal. Haematological and biochemical parameters were with in normal limits. Fiberoptic bronchoscopy revealed a dark, globular, smooth, fleshy growth covered with thick dark secretions about 2 cm below the vocal cords, occupying almost the complete tracheal lumen. The growth was extending about 2cm down wards into the trachea. It did not bleed on touch. Computerized Tomographic (CT) scan showed 2.2x2x1.4 cm oblong mass occupying the tracheal lumen, arising from the junction of lateral wall and posterior wall of upper trachea (Figure 1). No iymphadenopathy was detected. A cold nodule was also detected in the left lobe of thyroid. At this stage no probable diagnosis could be made. Surgery Open surgery was planned rather than a bronchoscopic removal. Due to the obstruction to the trachea, intubation during anaesthesia was difficult. Trachea was exposed by a vertical incision, slightly towards left of midline. Thyroid isthmus was transfixed and cut. Anterior tracheal wall was incised left of midline below the lower border of cricoid cartilage down to fifth tracheal ring. The growth was seen in the incision extending upwards in to the lumen on the right side and was attached to the right cricoid lamina by a broad base. To get a better view, the endotracheal tube was removed from the oral cavity and re-inserted directly into the tracheal lumen like tracheostomy tube. To access the base the incision was required to be extended on the right half of the trachea along the lower border of the cricoid. The friable mass was excised in toto, haemostasis secured and the tracheal incision was sutured leaving a gap just below the cricoid for the tracheostomy tube. The cold nodule in the thyroid was also excised. Tracheostome was closed on the fifth day. Subsequently radiotherapy of 4600 cGy/28 fr/6 weeks was given along with concomitant chemotherapy of cisplatin and docetaxel. She was reviewed three monthly after completion of concurrent chemo-radiotherapy and found to be in complete remission even after one year. CT scan after one year of surgery does not show any local recurrence (Figure 2) or any lymphadenopathy. Histopathological examination Tumour was received as three dark friable pieces, together measuring 2.8x2.5x1.5 cm. Microscopy revealed sheets and syncytial masses of large cells with ill-defined cell margins and large nuclei with 1 to 3 nucleoli (Figure 3). The tumour cells showed frequent mitoses. Areas of necrosis were seen. There were few scattered small lymphocytes among these large cells. Poorly differentiated carcinoma and lymphoma were the diagnoses entertained. Immunohistochemlstry showed that the large cells were cytokeratin positive and focal epithelial membrane antigen positivity was also seen. These cells were negative for S-100 protein and leucocyte common antigen. Malignant cells were negative for EBV genome by in-situ hybridization. Patient's serum had shown no significant titres of EBV Ig M antibodies by ELISA. The excised nodule from the thyroid was a cystic colloid nodule. DISCUSSION Lymphoepithelioma like carcinoma, originally described in the nasopharynx has been reported in other locations like thymus, parotid, uterine cervix, skin, breast, lung and upper aero-digestive tract.9 Commonest site is the nasopharynx where EBV is almost invariably associated. Elsewhere this association is variable.10 Association of EBV is consistent in Chinese where as it is lacking in Caucasians.5,11 Reports from India also show positivity for both type A EBV and type B EBV,12 while our case was negative. This tumour is characterized by the microscopic findings of a poorly differentiated carcinoma, causing diagnostic difficulty in differentiating from lymphoma. Histologically, lymphoepithelioma is the term used to describe an undifferentiated mucosal carcinoma with lymphocytic component. Immunohistochemistry is essential to differentiate this tumor from lymphoma. To our knowledge this is the second report of such case in the trachea. Previous reported case in trachea is in a seventy-one year old woman. Our case is in a young patient and the diagnosis was not considered before the surgery due to the young age of the patient and due to the rarity of this lesion in this site. Behavior of this tumour is highly variable ranging from apparent curability by excision to highly aggressive, extensive disease at presentation.13 Our case did not have any lymphadenopathy or extension of the disease beyond the trachea at the time of presentation and the patient is disease free after one year of treatment. The patient is on regular follow up to evaluate the efficacy of the treatment of surgery, radiotherapy and concomitant chemotherapy. This case is reported for its rarity especially in the trachea in a young individual and problems it can pose during anaesthesia, surgery and in the histological diagnosis. REFERENCES
Copyright 2002 - Indian Journal of Cancer. The following images related to this document are available:Photo images[cn02005f1.jpg] [cn02005f3.jpg] [cn02005f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}