 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
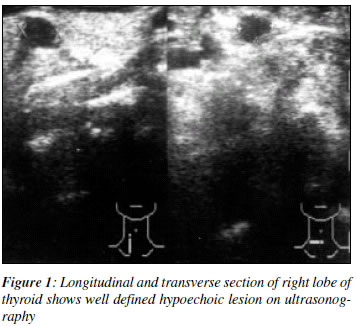
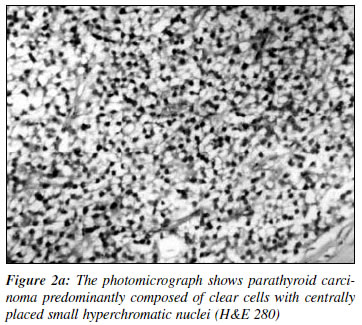
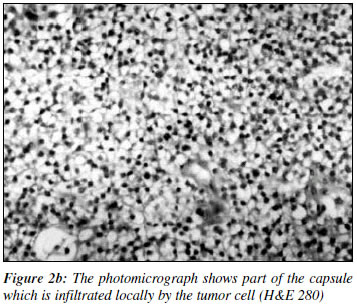
Indian Journal of Cancer, Vol. 39, No. 3, (July - September 2002), pp. 119-122 Parathyroid Carcinoma : Difficult Management Options A. Bhansali, R. N. Kataria, P. Dutta, M. M. Saha, P. Singh, R. J. Dash Department of Endocrinology, Postgraduate Institute of Medical Education & Research, Chandigarh 160 012. Code Number: cn02007 ABSTRACT Parathyroid carcinoma is a rare cause of primary hyperparathyroidism and these tumours are usually hyperfunctional as opposed to other malignant endocrine tumors. Surgery is the only effective treatment while nonsurgical modalities yield poor results. We report a patient, who presented with palpable mass in the neck and severe hypercalcemia. He underwent debulking surgery and received allendronate, calcitonin, dacarbazine followed by in- situ alcohol instillation with some success. Key Words: Hypercalcemia, Parathyroid carcinoma. INTRODUCTION Benign parathyroid adenoma is common compared to parathyroid carcinoma that comprises 0.5% to 4% of all patients with primary hyperparathyroidism.1 Virtually, all parathyroid carcinomas are functional in contrast to other malignant endocrine tumours.2 They usually present with severe hypercalcemia2 and variably respond to extensive enbloc resection,1 chemotherapeutic agents like adriamycin, decarbazine (DTIC),3 bisphosphonates;4 immunisation with PTH peptides,5 calcimimetic agents (NPS R568) 6 and non calcemic Vitamin D analogues.7 We report a patient, who presented with severe hypercalcemia, had debulking surgery and received allendronate, calcitonin, dacarbazine followed by in-situ alcohol instillation with some benefit. CASE REPORT A 40-year-old male with history of recurrent fractures (right clavicle and right femur neck) following trivial trauma during the past one year, was admitted with fracture of the left femur neck. He had progressively increasing hoarseness of voice, polyuria and constipation during last 6 months. He had no history of renal colic, graveluria, hematuria, acid peptic disease and neck irradiation. On examination, he was pale, emaciated and dehydrated. His pulse was 88/min, and BP 146/90mmHg. He had a 3x3cm firm, nodular, non tender swelling in relation to right lobe of thyroid and 2xlcm firm, right supraclavicular lymphnode. Both lower limbs were externally rotated. Other systemic examination was normal. Indirect laryngoscopy revealed right vocal cord palsy. On investigation, his hemoglobin was 9gm/dl, serum biochemistry including calcium ranged from 12.4 to 18.9 mg/dl (corrected for albumin), phosphate 2.4 to 3.5mg/dl, alkaline phosphatase 56 KA units, parathormone (intact)447 pg/ml (normal 5-72 pg/ml), creatinine 1mg/dl, sodium 138 mEq/L, kalium 4.6 mEq/L and random blood glucose 250mg/dl. His arterial blood gas and thyroid hormone profiles were normal. His 24 h urinary calcium was 625 mg, phosphate 840mg with creatinine of 1.1 gm. Skeletal X-rays revealed classical features of hyperparathyroidism including subperiosteal resorption in phalanx, cystic lesion in radius, pubic rami and skull bones with bilateral fracture of femur neck. Ultrasonography (US) of neck region showed 3x2xl.5 cm nodular lesion with loss of fat plane in inferior part of the right lobe of thyroid and 2.5x2xl cm in upper pole of the left lobe of thyroid (Figure l) Abdominal US showed nephrocalcinosis and hyperechoeic lesions in liver. Fine needle aspiration cytology (FNAC) from nodular lesion in neck was indicative of parathyroid carcinoma and from the hyperechoeic lesion of the liver suggested metastasis. Preoperatively, he was managed with IV saline, furosemide, calcitonin and allendronate and insulin for control of diabetes. After achieving euglycemia, he had tumour debulking with nodal resection. The tumour was infiltrating into right lobe of thyroid, tracheo-oesophageal groove and was extending to opposite side. Debulking surgery and hemithyroidectomy was performed. Histopapthology revealed parathyroid carcinoma (Figures 2a & 2b). Post-operatively, serum calcium decreased to 11.2 mg/dl but on day 2 it again showed rising trend. He was treated with dacarbazine 4mg/kg/day for 5 days and such two courses (at one month's interval) were given without much change in calcium profile. In view of the residual tumor and persistent hypercalcemia, ultrasound guided insitu instillation of absolute alcohol (3.5ml) was carried out, following which he developed left vocal cord palsy also. Tracheostomy was performed and dexmathasone was added to reduce laryngeal tissue edema. Subsequently serum calcium came down to 10.6 mg/dl, phosphate 4.8mg/dl, alkaline phosphatase 20KA units. Later patient was discharged on request but reportedly died 2 weeks later possibly because of aspiration. DISCUSSION Parathyroid carcinoma is usually hyperfunctional associated with high circulating levels of PTH (upto 5 fold), severe hypercalcemia, and renal (90%) and bone (70%) involvement.1 Upto 14% of patients with parathyroid carcinoma present with hypercalcemic crisis, manifesting as altered sensorium, dehydration and severe hypercalcemia (16mg/dl).8 Palpable neck mass in such a clinical setting is a strong pointer to parathyroid carcinoma and, in fact proven to be so in 22% to 50% of cases.1 Hoarseness of voice, due to compression or invasion of recurrent laryngeal nerve is reported in 10% of the patients.2 Our patient under report had classic presentation of parathyroid carcinoma with palpable mass in neck, hoarse voice, multiple fractures, bilateral nephrocalcinosis, high serum PTH and severe hypercalcemia (18.9 mg/dl). The clinical course of parathyroid carcinoma is variable but typically follows a pattern of local recurrence and later distant metastases to lung, bone and liver following tumour surgery. A few patients with parathyroid carcinoma have metastases either to regional lymphnodes (<5%) or distant sites (<2%) at initial presentation, as happened in our case.2 Surgery is the only effective treatment of parathyroid carcinoma.4 Preoperative diagnosis of parathyroid carcinoma facilitates decision for enbloc tumour resection and long term disease free survival.1 Decarbazine alone or in combination with 5-flourouracil and cyclophosphamide offer a favourable response only occasionally.3 The bisphosphonates, like etidronate and pamidronate has also been used with some success.4 Allendronate 10 times more potent than pamidronate, was preferred (30mg/day) in this case even prior to debulking but with not much change in calcium profile. Because of extensive disease, our patients had only debulking surgery followed by 2 courses of dacarbazine at one month interval with insignificant decrease in serum calcium. In-situ absolute alcohol instillation has been used in the management of parathyroid adenoma with transient benefit over 6 months.9 However, its use in patients with parathyroid carcinoma has not been reported. Following in- situ alcohol instillation in our patient his serum calicum fell to 10.6 mg/dl. Recurrent laryngeal nerve injury following this procedure which he had, has been reported in rare instances.9 Recently calcimimetic agent (NPS R568) has been used in a case of recurrent parathyroid carcinoma with success.6 Serial measurement of calcium and / or PTH serve an ideal tumour marker and in most cases hypercalcemia precedes the physical evidence of recurrence. Long term survival in patients with parathyroid carcinoma ranges between 18% and 78% in various series. A summary of 251 patients showed a 5 year survival rate of 57% and 10 year survival rate of 39%.10 Persistent hypercalcemia following initial surgery is a poor prognostic indicator as 60% of patients died within 3 years. REFERENCES
Copyright 2002 - Indian Journal of Cancer. The following images related to this document are available:Photo images[cn02007f1.jpg] [cn02007f2a.jpg] [cn02007f2b.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}