 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
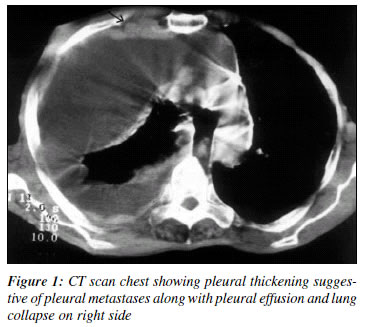
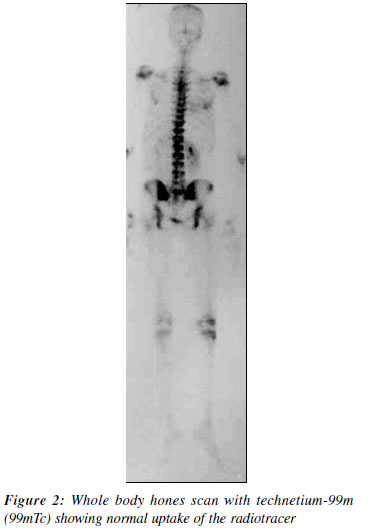
Indian Journal of Cancer, Vol. 39, No. 3, (July - September 2002), pp. 123-124 Massive Pleural Effusion without Bony Involvement: An Unusual Presentation of Advanced Carcinoma Prostate M. S. Ansari, Gholam Nabi, Amlesh Seth Department of Urology, All India Institute of Medical Sciences, New Delhi 110 029. Code Number: cn02008 ABSTRACT As noted under the natural history, the bone of axial skeleton and the ileopelvic lymphnodes specially the obturator groups are the commonest sites of metastasis spread of cancer prostate. Visceral metastasis in the absence of the above is extremely rare. We present a 50-year-male patient of cancer prostate with pleural metastases, pleural effusion and lung collapse on right side. Bone scan was essentially normal. Bilateral orchiectomy was done. Pleural effusion subsided and PSA dropped to 1.4 ng/ml from the initial 120 ng/ml at three months. Patient is on regular follow-up at three monthly intervals and last PSA done at 9 months was 2.1 ng/ml. CASE REPORT A 50-year-male patient presented with breathlessness and lower urinary tract symptoms (LUTS). Clinical examination revealed right side absent breath sounds and digital rectal examination showed a hard nodular prostate. Serum PSA was 120 ng/ml. X-ray chest showed right side pleural effusion with lung collapse. CT scan chest showed pleural thickening suggestive of pleural metastases along with pleural effusion and lung collapse on right side (Figure 1). Trucut biopsy prostate showed adenocarcinoma prostate. C.I. guided biopsy of pleural nodule was compatible with metastatic prostate cancer. The whole body bones scan with technetium-99m (99mTc) showed normal uptake of the radiotracer (Figure 2). Pleural tape was performed which provide symptomatic relief to the patient. Subsequently, bilateral orchiectomy was done. Pleural effusion subsided and PSA dropped to 1.4 ng/ml al three months. Patient is on regular follow-up al three monthly intervals and last PSA done at 9 months was 2.1 ng/ml. DISCUSSION The prognosis of prostate cancer is mainly determined by the presence or absence of metastases. The bones of axial skeleton sire a frequent site of metastatic spread of carcinoma prostate. Spine metastases precede the lung and liver metastasis. Pleural involvement without the Involvement ob bone is extremely rare. Review of literature shows that the pleural involvement is the second rarest site after the adrenals among the soft tissue metastases.1 Androgen ablation therapy is the treatment of choice for the palliation of patients with advanced prostate cancer. Maximal androgen ablation (MAB) (combination of medical or surgical castration and an antiandrogen) has been shown to increase the survival of patients with metastatic prostate cancer specially in low volume disease and patients with good performance status. More recent data show that orchiectomy alone is as effective as MA13 in advanced stage cancer with similar palliation and survival.2 Cytotoxic chemotherapy has been attempted in patients with metastatic adenocarcinoma with or without hormone insensitivity. Cytotoxics chemotherapeutic agents have also been tried in conjunction with endocrine therapy, however, no survival advantage has been demonstrated.3 In patients with hormone refractory prostate cancer with symptomatic bone metastases, palliation can be achieves with either selective external been radiation therapy a (XRT) to the metastases or administration of strontium- 89 (89Sr) or Phosphorous 32 (P32). We feel that local radiotherapy should he avoided in patients with pleural effusion even if associated with bony rib metastasis as it might aggravate the lung fibrosis, which is already collapsed due to effusion. Initial trial of hormonal manipulation with either orchiectomy or LIIRI-I analogues (with an antiandrogen for initial 2-3 weeks) alone is a prudent step. In case of PSA not returning to normal value or rising PSA other modalities can be tried. REFERENCES
Copyright 2002 - Indian Journal of Cancer. The following images related to this document are available:Photo images[cn02008f2.jpg] [cn02008f1.jpg] |
| |||||||||

{kind=link}
{kind=link}