 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
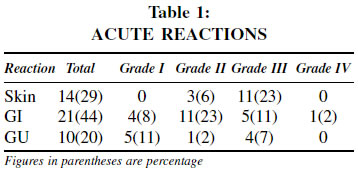
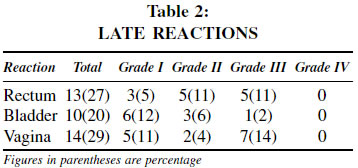
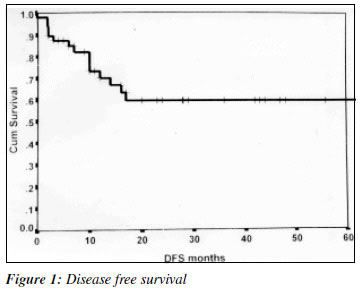
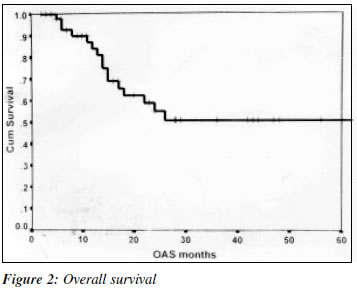
Indian Journal of Cancer, Vol. 39, No. 4, (October - December 2002) , pp. 127-134 Hypofractionated Radiotherapy in Carcinoma Cervix IIIB Tata Memorial Hospital Experience Mary A. Muckaden, Ashwini N. Budrukkar, Hemant B. Tongaonkar, Ketayun A. Dinshaw Dept. of Radiation Oncology, Tata Memorial Hospital, E. B Marg, Parel, Mumbai 400 012, Maharashtra. Code Number: cn02009 ABSTRACT PURPOSE OF THE STUDY: To analyze the role of hypofractionated radiotherapy in advanced carcinoma of cervix. BASIC PROCEDURE: Medical records of 62 women with advanced carcinoma cervix III3 treated during 1994-1996 were reviewed. Patients were treated with standard pelvic portals to a total dose of 39Gy in 13 fractions over 17 days followed by intracavitary brachytherapy. Forty-eight patients completed the planned treatment and were considered suitable for analysis of late reactions and survival. MAIN FINDINGS: The 5-year disease free survival was 59% and the overall survival was 50% at the mean follow up of 40 months. Twenty-one (44%) patients developed acute gastrointestinal toxicity of which 5 patients had grade III and one patient had grade IV reaction. Ten patients (21%) developed acute genitourinary complications, 13 patients (27%) had late rectal reactions and 10 patients (20%) had late bladder complications. Three patients had grade I, five had grade II and five had grade III late rectal toxicity. CONCLUSION: Survival in patients treated hypofractionated radiotherapy appears comparable to that of standard fractionation. The acute gastrointestinal and skin reactions were mainly grade I or grade II. Hypofractionated radiotherapy can certainly be considered in a select group of patients where the local disease is extensive and is unsuitable for conventional treatment. Key Words: Hypofractionation, Cancer cervix, Radiation Therapy. Introduction Carcinoma of cervix is one of the most common gynaecological malignancies in India. Even though cancer screening has become prevalent with an aim of early diagnosis and treatment, about 60% of the patients still present in late stage.1 Radiation therapy plays important role in carcinoma cervix stage II, III and IV.2,3 As per Tata Memorial Hospital cancer registry 88% of the patients receive radiation therapy as the single modality treatment. Treatment for carcinoma cervix stage IIIB is a combination of external beam radiation and brachytherapy. Conventional external beam radiation delivers a dose of 2Gy per fraction with standard pelvic portals with antero-posterior or box field technique. Time dose and fractionation schedules have been altered in an attempt to improve the probability of local control.4 Various altered fractionation schedules include hypofractionation, rapid fractionation, split course regimen, hyperfractionated and accelerated hyperfractionation. Hypofractionated radiotherapy delivers high dose per fraction (>2-2.5Gy), daily for 5 days with a gap of 24 hours. Reduction in the total dose is needed taking into consideration high dose per fraction so as to reduce the normal tissue effects. The treatment time and number of fractions is hence reduced. At few centres hypofractionated radiotherapy has been delivered twice weekly or four days a week. Hypofractionated radiotherapy has been considered at a few centers for palliation. Various studies with split course radiation therapy have also practiced hypofractionation.5 Overall treatment time has considerable effect on local control and survival. In hypofractionated treatment the overall treatment time is reduced. But the beneficial effect of reduction in overall treatment time is counteracted by high dose per fraction. The chances of late complication increase with increasing dose per fractionation. Alteration in the fractionation has been attempted mainly to improve the local control at the same time decreasing the normal tissue complications.6 Carcinoma cervix stage IIIB includes a heterogeneous group of patients of small volume disease to extensive disease with bilateral parametrial involvement upto lateral pelvic wall. Some of these patients do not have good general condition and hence are not suitable for 4-5 weeks of external radiation. These patients were considered for hypofractionated radiotherapy at our centre. We review our experience with hypofractionated radiotherapy. An analysis of all the patients of carcinoma cervix stage IIIB who received hypofractionated external beam radiation therapy was carried out with aims to assess the efficacy of hypofractionated radiotherapy, to assess the early and late complications related to the treatment. The disease free and overall survivals were also calculated. PATIENTS AND METHODS Medical records of 62 women with advanced carcinoma cervix IIIB treated during 1994-1996 were reviewed. Mean age of presentation was 49 years (range 30 to 62). Ninety percent of the patients had bleeding per vaginum as their main complaint while remaining 10% had white discharge. Patients also had associated symptoms like backache, abdominal pain and weakness. The mean duration of symptoms was 5 months (range 1 to 36 months). These patients were jointly evaluated by surgical and radiation oncologist. Thirty two patients had bulky cervical disease (>4cm) while 30 patients had moderate lesion over cervix. Forty two patients had upper one third vaginal involvement while 20 patients had upper two third vaginal involvement. Histopathology was epidermoid carcinoma in 56 (90%) patients, adenocarcinoma in 4 (7%) patients and adenosquamous in 2 (3%) patients. After staging and investigations they were considered for radiation therapy. Hypofractionated radiotherapy was considered due to extensive local disease and general condition of the patients. Thirty-seven (60%) patients were treated with telecobalt while 25 (40%) patients were treated with linear accelerator. Patients were treated with standard pelvic portals with anteroposterior or box field technique. The dose per fraction was 300cGy per fraction in which all fields were treated per day. The patients were treated for 5 days a week and the total dose delivered was 39Gy in 13 fractions over 17 days. Patients were assessed during radiation therapy for acute genitourinary, gastrointestinal and skin reactions. After completion of external radiation patients were considered for intracavitary brachytherapy. Intracavitary application was feasible in 44 patients while in 4 patients it could not be done due to extensive local disease. These patients were treated symptomatically. Thirty five patients were treated with standard intracavitary application with central tandem and two ovoids delivering a dose of 25Gy to point A. Four patients were treated with central tandem and vaginal cylinders to a dose of 15Gy to point A. Three patients received 10Gy with vaginal surface applicator while two patients were treated with central vaginal source delivering 15Gy at 0.5cm from the surface of the cylinders. Patients were followed up at 6 weeks of completion of radiotherapy, three monthly for the first year, 4 monthly for the second year and 6 monthly thereafter. At each follow up patients were assessed for late reactions of skin, vagina, rectum and bladder. Patients who had bleeding per rectum were treated symptomatically. In patients where bleeding was not controlled even after symptomatic management were considered for sigmoidoscopy. These patients were then treated with steroid enema. Patients who had evidence of local disease at 6 weeks of completion of treatment were considered to have persisting disease. Patients were considered to have recurrence when disease was seen after initial complete response. Patients who had persisting disease or recurrence were considered to have locoregional failures. Early and late reactions were assessed according to the RTOG scale. Statistical analysis was performed using SPSS for Windows and Kaplan Meier method was used for calculating the survival.7 RESULTS Acute Reactions Skin Fourteen (29%) patients developed acute skin reactions. Three (6%) patients had grade II skin reaction and 11 (23%) patients had grade III skin reaction in the form of moist desquamation (Table 1). One patient developed moist desquamation after two weeks of starting radiation therapy. She required admission in the ward for supportive care. Skin reaction was treated with gentian violet 1 % and the radiation was completed. Nine patients developed moist desquamation after 3 weeks and one patient developed at 4 weeks of starting radiotherapy. All these patients were managed conservatively. Gastro intestinal Twenty-one (44 %) patients developed acute gastro intestinal reactions during radiation therapy. Out of these 4 patients had grade I reaction and eleven (23%) had grade II reaction. Six patients (12%) developed severe gastro intestinal toxicity. Five patients had grade III reactions while one patient had grade IV reaction. Two patients developed gastro intestinal toxicity at two weeks. They were treated with anti-motility agents and plenty of fluids orally. Two patients required in patient care for the gastro-intestinal reactions. Inspite of the reactions all the patients completed the planned radiation therapy. Rectal reactions Ten (21%) patients developed genitourinary complications during treatment. Out of these 5 patients developed grade I proctitis, one patient developed grade II proctitis while 4 patients developed grade III proctitis. Two patients developed bleeding per rectum during treatment of which one developed at 2 weeks and the other at 3 weeks of starting radiation. In one patient radiation had to be stopped due to proctitis. This dose was compensated by giving higher intracavitary dose. These patients were managed successfully with anti-inflammatory agents and steroid enema. Late Complications Among the late complications bladder and rectal were the main severe complications that were observed. Vaginal stenosis was another complication that was observed in these patients (Table 2). Rectal reactions Thirteen (27%) of the patients developed late rectal reactions. Three patients had grade I, five had grade II and five had grade III rectal toxicity. The mean duration of appearance of symptoms was 13 months with a range of 7-30 months. Sigmoidoscopy revealed telengectasia from anal verge upto 15-20 cm in these patients. All the patients were initially treated with anti-inflammatory drugs. If they did not respond to anti-inflammatory drugs, steroid enema was considered. Enema was given as steroid retention enema of 100mg of hydrocortisone given in 100ml of normal saline, twice daily for 15 days. Two patients had profuse bleeding per rectum and required in patient care. These patients required blood transfusions to achieve stable hemodynamics. One patient was advised colostomy but refused. Five patients continued to have bleeding per rectum till their last follow up. Once the reaction developed it continued for an average of 13 months. Bladder reactions Late bladder complications were observed in 10 (20%) of the patients. Six patients had grade I reaction, 3 had grade II and 1 patient had grade III bladder toxicity. Average duration of presentation was 27 months with a range of 6 to 57 months. All the patients were managed conservatively and were controlled. Vaginal stenosis Though vaginal stenosis was not the main presenting symptom in any of the patient, it was a significant finding in 14 (30%) of the patients. Five patients had vaginal synechia, 2 had vaginal narrowing while seven patients had vaginal stenosis. Only one patient had dyspareunia. One patient had vulval edema along with vaginal stenosis. Survival At six weeks after completion of radiation therapy 41 (85%) patients achieved complete response, two patients had partial response, two had no response while three patients had progressive disease on follow up. Three patients who had progressive disease continued to have persistent disease. Six patients developed central recurrence. Four patients developed distant metastasis in bones, supraclavicular region, liver and lung each. Out of the four patients with distant metastasis two patients also had locoregional failure. The 5-year disease free survival was 59% and the overall survival was 50% (Figures 1& 2). The mean follow up was 40 months. DISCUSSION Conventional fractionation delivers 1.8-2Gy per fraction 5 days a week. This fractionation scheme was developed because of tolerable acute reactions, acceptable delayed effects and reasonable local controls. In an attempt to improve the therapeutic ratio various fractionation schedules have been attempted. Hypofractionation has been used in various head and neck, bladder and gynecological malignancies.8-10 Lee et al studied 23 patients with stage III and IV head and neck carcinomas treated with 44-52Gy/11-13 fractions. The actuarial survival rate at 2 years was 45% and local control was 59%.8 Fraction size is the dominant factor in deciding the late effects. Increase in the dose per fraction also causes increase in the late effects. Carcinoma cervix is one of the most common gynecological malignancies in India. Large number of patients present at late stages due to various reasons. Carcinoma cervix stage IIIB forms a heterogenous group of patients ranging from small volume disease with bilateral parametrial involvement upto lateral pelvic wall to extensive disease with bulky parametrial involvement. A subgroup of these patients in whom there is extensive local disease at presentation, have fair general condition and who cannot withstand 5 weeks of standard treatment were considered for hypofractionated radiotherapy. Eighty five percent of the patients achieved complete response after completion of radiation therapy, which is comparable to that of conventional treatment. Recurrence rate of 12.5% is comparable to that seen in other series in patients with carcinoma cervix IIIB.2,3 The rate of distant metastasis was 8% in our study. Surprisingly the tumor control and the disease free survival were comparable to the conventional treatment.2,3,11-13 The disease free survival in carcinoma cervix IIIB ranges from 40-60%.2,3,11-13 The disease free survival of 59% seen in our series is comparable to that of conventional fractionation. As we would have expected this treatment was moderately tolerated by the patients. Mild gastrointestinal toxicities were observed in 43% of the patients. Five patients had grade III reactions while one patient had grade IV toxicity. Two patients required in patient care during treatment. Thus most of the patients had mild radiation reactions. Twenty- percent patients had acute genitourinary toxicity. Two patients developed bleeding per rectum on treatment. Acute proctitis was translated into late consequential effect in these two patients as these patients continued to have bleeding per rectum after completion of treatment on follow up. Skin reactions were observed in 29% patients. Eleven patients had grade III skin reaction and were treated symptomatically. Twenty seven percent of the patients developed late rectal reactions in our study. Eight patients of these had early i.e. grade I and II rectal reactions while 5 patients had grade III rectal reactions. Radiation proctitis is one of the troublesome complications after pelvic radiotherapy.13-18 The clinical manifestations vary from rectal proctitis, stricture, bleeding ulcers and fistula formation. The rate of late rectal morbidity has been reported as between 2-25% of the patients.19 The rate of complications observed in our study was slightly on the higher side when compared to that of the literature. Bleeding can be severe in many patients leading to repeated transfusions and anemia. The time of development of bleeding has been reported between 6 months to one year after completion of radiation therapy and is caused by friable mucosal angioectasias.20 Yegappan et al have reported mean duration of 19.9 months after radiotherapy.21 We have found that the bleeding developed at an average of 13 months of completion of radiation therapy. Two patients who had acute radiation proctitis continued to have bleeding after treatment as a consequential late effect. In one patient the time of development was found to be as long as 30 months. The correlation of proctitis with dose delivered has also been reported. Perez et al observed that when the dose delivered was below 75Gy the incidence of proctitis was <4% and it increased to 9% with higher doses. Treatment options for radiation proctitis vary from non steroidal anti inflammatory drugs, steroids enemas to various surgical techniques.22 Local application of formalin and sucralfate enemas have been used.23 Argon plasma coagulation is one of the new techniques for the treatment of radiation proctitis.24,25 Surgical techniques have been used in patients with chronic radiation proctitis.21 If surgery is necessary, a transverse or descending colostomy should be tried. Aggressive surgery such as rectal resection and colo-anal anastomosis is associated with significant morbidity and mortality and should be reserved as last measure. We have treated our patients with anti-inflammatory drugs and steroid enemas. Once the reaction developed it continued for an average duration of 13 months. Five patients continued to have bleeding till the last date of follow up. One patient was advised colostomy but refused. Radiation cystitis is observed in 6-15% patients receiving pelvic radiotherapy.26-28 Clinical picture varies from repeated urinary tract infections, burning micturation, hemorrhagic cystitis, stricture formation to fistula formation. The treatment modalities include antibiotics, urinary alkalizers, alum or formalin instillation, hyperbaric oxygen and surgical techniques.29-32 Few patients may present with repeated bleeding leading to anemia and requiring blood transfusions. The incidence of severe hemorrhagic cystitis is relatively low. Minor episodes of hematuria can be managed by antibiotics and urinary alkalizers. Cystoscopy should be reserved for patients with repeated bleeding. These patients can be managed with clot evacuation and continuos bladder irrigation. Patients who do not respond to this conservative approach are treated with alum instillation.29 Intravesical instillation of 1% alum or 4% formalin have been found to be effective in treating intractable hematuria.32 Hyperbaric oxygen therapy has also been used in patients with intractable radiation cystitis.30 In our series 20% patients had cystitis of which 18% patients had mild (grade I/II) cystitis. Only one patient had grade III cystitis. This patient had severe hematuria, passed clots in urine but recovered with conservative management with irrigation of bladder. The mean duration of symptoms was 27 months, which was comparable to that in other series.30 CONCLUSION Hypofractionated radiotherapy for advanced carcinoma cervix stage IIIB gives survival comparable to that of standard treatment. Though the acute as well as late radiation sequelae seem to be higher they are mainly grade I/II reactions. Percentage of patients developing severe radiation sequelae is comparable to that of standard treatment. Hypofractionated radiotherapy can be considered in a select group of patients where local disease is extensive and hence unsuitable for conventional fractionation. REFERENCES
Copyright 2002 - Indian Journal of Cancer. The following images related to this document are available:Photo images[cn02009t1.jpg] [cn02009t2.jpg] [cn02009f1.jpg] [cn02009f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}