 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
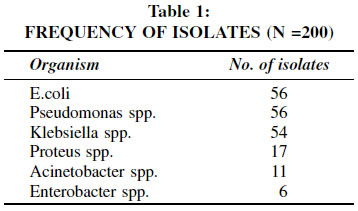
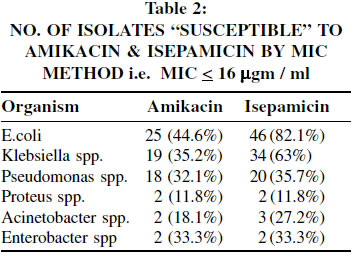
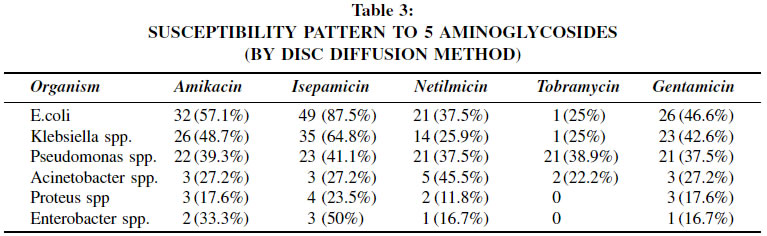
Indian Journal of Cancer, Vol. 39, No. 4, (October - December 2002) , pp. 135-138 Invitro Comparative Evaluation of Aminoglycosides at a Cancer Centre S. K. Biswas, R. S. Kelkar Dept. of Microbiology, Tata Memorial Hospital, Parel, Mumbai 400 012. Code Number: cn02010 ABSTRACT A comparative study of in vitro activity of amikacin, gentamicin, netilmicin, tobramycin and isepamicin was done. A total of 200 clinical isolates of Gram negative organisms from various clinical sources were tested. E.Coli was the most frequently isolated organism followed by Pseudomonas spp., Klebsiella spp., Proteus spp., Acinetobacter spp. and Enterobacter spp. Of the 5 aminoglycosides tested, isepamicin showed the highest numbers of susceptible isolates followed by amikacin, netilmicin, gentamicin and tobramycin. MIC 90 value of isepamicin was lower as compared to amikacin. Key Words: Isepamicin, Aminoglycosides, MIC. INTRODUCTION Gram-negative infections remain a serious cause of morbidity and mortality in cancer patients. Empiric treatment protocols at our centre have always included an aminoglycoside. This was earlier gentamicin. Current protocols include amikacin in combination with a third generation cephalosporin. The incidence of multi drug resistant microorganisms has however become a serious threat to the management of infectious complications of cancer. The aminoglycosides continue to be useful antibiotics for the treatment of serious Gram-negative infections despite their narrow therapeutic index.1 However, bacterial resistance to the aminoglycosides through the acquisition of aminoglycoside inactivating enzymes is an increasing problem where aminoglycoside usage is prevalent.2 Isepamicin is a novel, broad-spectrum aminoglycoside which possesses a high level of stability to aminoglycoside inactivating enzymes and low level of toxicity.3 The spectrum of isepamicin activity includes all species of Enterobacteriaceae, Pseudomonas spp., many strains of Acinetobacter spp., and majority of Staphylococci. The level of activity of isepamicin is similar to that of amikacin.3 Like other aminoglycosides, isepamicin acts by binding bacterial ribosomes. The binding results in the misreading of mRNA and ultimately cellular death via inhibition of bacterial protein synthesis.4,5 Aminoglycoside resistance in clinical isolates is most often caused by three types of aminoglycoside - modifying enzymes, which either utilise acetyl-CoA to acetylate amino groups or adenoside triphosphate to phosphorylate or adenylylate hydroxyl groups.6 Isepamicin has predictable pharmacokinetics and is similar to most other aminoglycosides in its physicochemical and pharmacokinetic properties.7 The present study was undertaken to evaluate the in vitro efficacy of isepamicin in cancer patients and compare it with amikacin, gentamicin, tobramycin and netilmicin. This included evaluation both by Kirby- Bauer's disc diffusion method and determination of minimum inhibitory concentration (MIC) by agar dilution method. PATIENTS AND METHODS 200 clinical isolates obtained during January 2000 to April 2000 from cancer patients admitted to the Tata Memorial Hospital were included in this study. These clinical isolates were obtained from blood, pus, urine, sputum, body fluids, intravenous catheters etc. The bacterial isolates were identified by standard microbiological methods. Antibiotic susceptibility testing for all the aminoglycosides studied was done by Kirby Bauer's disc diffusion method. For isepamicin, 30 mgm discs (Fulford India Ltd.) were used. Zone diameters used for interpretation was < 14mm as resistant, 15-16 mm as intermediate and > 17mm as sensitive. The zone diameters for interpretation of the other aminoglycosides was as per the NCCLS guidelines. The agar dilution method was used for MIC determination of amikacin and isepamicin. The range of concentrations for both isepamicin and amikacin was 2 to 64/4 mgm/ml. The end point is the concentration of drug completely inhibiting the growth of the organisms.8 The interpretation was based on the criteria laid down by the NCCLS.8 Staphylococcus aureus (ATCC 29212), Escherichia coli (ATCC 25922) and Pseudomonas aeruginosa (ATCC 27853) obtained from the American Type Culture Collection (Rockville, USA) were used along with the antimicrobials in accordance with NCCLS recommendation.8,9 The end-point MIC concentration used for interpretation of isepamicin was < 16 mgm/ml as sensitive, 32 mgm/ml as intermediate and > 64 mgm/ml as resistant. RESULTS Two hundred isolates were included in this study. There were 56 isolates of E.coli and Pseudomonas spp. each, 54 were Klebsiella spp, 17 were Proteus spp., 11 were Acinetobacter spp. and 6 were Enterobacter spp.(Table 1). 107 of the isolates were susceptible to isepamicin and 68 to amikacin by disc diffusion method which was confirmed by the agar dilution method (Table 2).The susceptibility patterns to 5 aminoglycosides that were tested by Kirby-Bauer's method is shown in (Table 3). DISCUSSION Two hundred isolates were tested. Isepamicin susceptible isolates were 107 whereas 68 isolates were susceptible to amikacin by the disk diffusion technique as well as with agar dilution method (Table 2). Of the susceptible strains, 59 strains showed an MIC <4 to isepamicin whereas for amikacin, the same was true for only 33 strains. 77 strains were susceptible to gentamicin, 64 to netilmicin and 25 to tobramycin by disc diffusion method. Gentamicin use (as a part of the treatment regimens at Tata Memorial Hospital) has been discontinued in the late 80's.However,this has shown some improvement in susceptibility patterns but not significant enough to warrant clinical use. In our experience, netilmicin was found to be useful for the management of Acinetobacter species infections and infections with methicillin resistant Staphylococcus aureus. Results of in vitro testing with tobramycin have never been encouraging enough to warrant its clinical use. Isepamicin showed a superior in vitro activity as compared to other aminoglycosides. This observation from the present study suggests that isepamicin is more potent against certain commonly occuring pathogens in a hospital environment as is also observed in other clinical studies.10,11 These studies showed that isepamicin administered at a dose of 7.5mg/kg twice daily for upto 14 days was as effective as amikacin at the same dosage for different bacterial infections in both neutropenic and non-neutropenic patients. Resistance to aminoglycosides is most often caused by the production of aminoglycoside inactivating enzymes. Isepamicin is a 1-Nacvl derivative of gentamicin B which is protected against aminoglycoside modifying enzymes. The only two aminoglycoside modifying enzymes .-KPH (3)-VI and ANT (4)-I or II and permeability mutation produce resistance to isepamicin. Isepamicin appears to be an aminoglycoside similar to amikacin. but with superior modifying enzyme stability and low nephrotoxicity and ototoxicity.4 These antimicrobial features of isepamicin may extrapolate to its expanded clinical use in hospitals where amikacin and other aminoglycoside resistance have become endemic. The use of isepamicin with other classes of drugs should be considered, especially for high risk areas. ACKNOWLEDGEMENT This study was supported by a clinical grant from Fulford India (Ltd.). We acknowledge the technical support rendered by Mrs. Lina Lakhani, Mrs. Charu Mathure and Mrs. Madhura Tungare. REFERENCES
Copyright 2002 - Indian Journal of Cancer. The following images related to this document are available:Photo images[cn02010t3.jpg] [cn02010t2.jpg] [cn02010t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}