 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
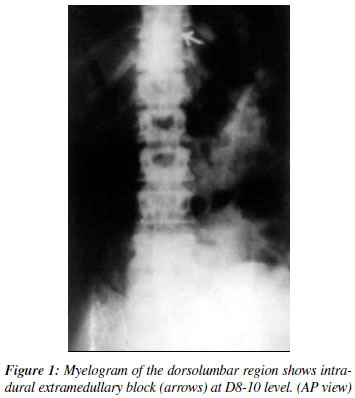
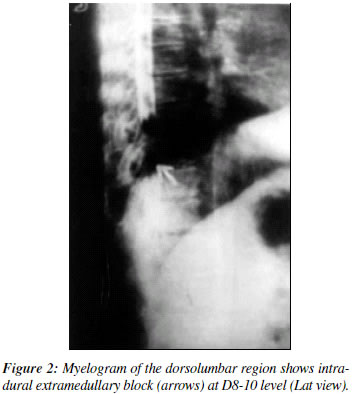
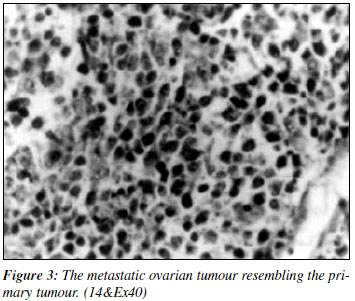
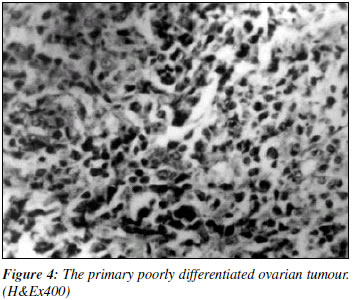
Indian Journal of Cancer, Vol. 39, No. 4, (October - December 2002) , pp. 157-160 Intradural Extramedullary Spinal Metastasis from an Ovarian Carcinoma Ravi Mehrotra, Kartikeya Sharma Department of Pathology, Motilal Nehru Medical College, 16/2, Lowther Road, Allahabad 211 002. ABSTRACT Intradural extramedullary metastases from tumours are a rare occurrence, accounting for less than 2 percent of all spinal metastases. We report a patient who presented with progressive paraparesis one and a half years after being operated for an poorly differentiated serous cystadenocarcinoma. Tumour mass decompression was carried out and the intradural tumour metastasis was removed. Histopathology revealed an identical appearance to the original ovarian tumour. This is the first reported case of an intradural extramedullary metastasis from a poorly differentiated serous cystadenocarcinoma of the ovary. Key Words: Ovarian tumour, Intradural, Extramedullary, Metastasis. INTRODUCTION Spinal Cord or cauda equina compression from a secondary deposit frequently complicates advanced cancers. It is the second most common neurological complication of cancer after brain metastases. At autopsy, its occurrence is documented in approximately 5% of patients with malignancies and inexorably results in cord compression.1 Compression of the spinal cord and / or its roots by extradural metastasic deposits is rarely seen - with a reported incidence of 1 to 4 percent in the literature.2-4 Intramedullary spinal cord metastasis has been reported to account for 2 percent of all spinal metastasis.2 We report a case of intradural extramedullary spinal cord metastasis from a patient with an ovarian carcinoma. CASE REPORT A 46-year-old female was operated for an ovarian tumour. Histopathological examination of the mass revealed poorly differentiated serous cystadenocarcinoma of the ovary. She was treated by panhysterectomy followed by full chemotherapy. One and a half years later, she presented with progressive painful paraparesis of three months duration. Within two days of admission, she developed complete paraplegia along with bladder and bowel dysfunction with sensory loss at Dorsal 6 vertebral level. She had severe excruciating pain, in addition to paraesthesia, in spite of regular analgesic (nonsteroidal anti inflammatory) drugs. Her haematological and biochemical investigations were within normal limits, except marked anaemia (8 gm. %) and hypoproteinemia. Her chest X-Ray and ultrasonographic examination of the abdomen were normal. Plain X-ray of the dorsolumbar region was inconclusive. Myelogram showed an intradural extramedullary block in the region of the Dorsal 8-10 vertebrae (Figures 1& 2). MRI could not be done as the patient was claustrophobic and did not agree to the procedure. She was operated upon under general anaesthesia and a midline dorsolumbar laminectomy was done. Extradurally, there was no pathology. On opening the dura, in the midline, a vascular greyish pink sheet of tumour was present underneath the dura, encircling the cord from the posterior and lateral aspects. Nerve roots in the cauda equina zone were engulfed with the tumour mass. Tumour mass decompression could be done without injuring the cord and roots. The dura was closed with interrupted sutures after obtaining free flow of CSF. Histopathology of the tumour mass showed a poorly differentiated serous cystadenocarcinoma of the ovary with features similar to the previously diagnosed ovarian tumour (Figures 3 & 4). A skeletal survey and routine liver and renal function were within normal limits. Postoperatively the patient had a significant reduction in pain and her power returned to grade-II. After three weeks of hospital stay she was transferred to the Oncology unit for radiotherapy. Patient was lost to follow-up thereafter as she did not turn up for check-up. DISCUSSION Metastatic deposits from solid tumours that seed in an intradural extramedullary fashion in the spinal cord are rare. The incidence of this pattern is likely to gradually increase in the near future as palliative and non-curative therapies for malignancies evolve and the population continues to age. Metastatic intradural extramedullary tumour can arise from either CNS or extra CNS sources. Extra-CNS tumours that are known to metastasise intradurally in this extra medullary fashion are cancer of the lung, breast, melanoma, lymphoma and leukaemia.5 Glioblastoma, anaplastic astrocytoma, medulloblastoma, pineal body tumour and choroid plexus tumours are the common CNS tumours that metastasise to the spinal subarachnoid space.6 Bone metastasis has been reported in a granulosa cell tumour of the ovary.7 Spinal metastasis can be intramedullary, leptomeningeal or epidural. Extradural are commonest, leptomeningeal are rare and intramedullary metastases are anecdotal5. The first case of intradural extramedullary metastasis was reported form a primary carcinoma of the adrenal.8 Regarding spread of primary tumours, absence of intra parenchymal lesions, choroid plexus metastasis or paravertebral tumours in such patients make haematogenous spread of tumour the most likely possibility. Once the tumour has seeded, it may grow in a linear fashion creating a thin layer of cells spread diffusively over the brain and spinal surface or may assume a nodular growth pattern in a multifocal skip lesion fashion with intervening tumour free areas.5 The interval from diagnosis of the primary malignancy to the spinal cord compression varies widely, with different tumours. In lung cancer, this spread may take a few days to a few months and is more than a decade in case of breast malignancy. Uncommonly tuberculosis has been reported to cause intradural extramedullary spinal cord compression.9 Clinical presentation depends upon the level of involvement. Early symptoms are non-specific like low backache, paraesthesia and gait disturbances etc. Monoparesis or paraparesis, with or without, bladder and bowel involvement can be the presenting symptoms. Signs and symptoms progress rapidly from few days to few months. In all such cases lumbosacral area is the most frequent site but the thoracic region may be involved too. Multiple lesions are common.1 Lesions are either diffuse sheet like infiltration or form a neoplastic coating of cord conus and cauda equina or may be nodular deposits scattered through out the subarachnoid space. CSF cytology is positive in about 75% of the cases. Myelography and CT Myelography may show following four major patterns:5 1) Nodular or plaque like deposits
intimately related to cord conus or cauda equina. MR may show iso-indense masses, which enhance dramatically after contrast and thin extension along nerve roots can also be demonstrated.10 The treatment protocol of these patients is not clear since no controlled trials are available in the literature. But early clinical diagnosis and vigorous treatment with surgery, radiotherapy and chemotherapy should be started to relieve symptoms and prevent progression. However, most of the patients either fail to respond or relapse within a short duration of the initial treatment. Overall prognosis is poor. Death generally occurs within four months in more than 80% of cases.11 Unfortunately our patient was lost to follow-up. Literature search indicated that this is the first reported case from a poorly differentiated serous cystadenocarcinoma of the ovary metastasising to the spinal cord. It should be kept in mind in the differential diagnosis of extramedullary tumour deposits. REFERENCES
Copyright 2002 - Indian Journal of Cancer. The following images related to this document are available:Photo images[cn02016f4.jpg] [cn02016f1.jpg] [cn02016f2.jpg] [cn02016f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}