 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 40, No. 1, (January - March 2003) , pp. 23-26 Atypical Squamous Cells of Undetermined Significance: Is It Worthwhile to Qualify Them Further? Sodhani P, Gupta S, Sehgal A,* Singh V,** Khan IU, Mitra AB*** Departments of Cytopathology, *Epidemiology, **Clinical Research and ***Molecular
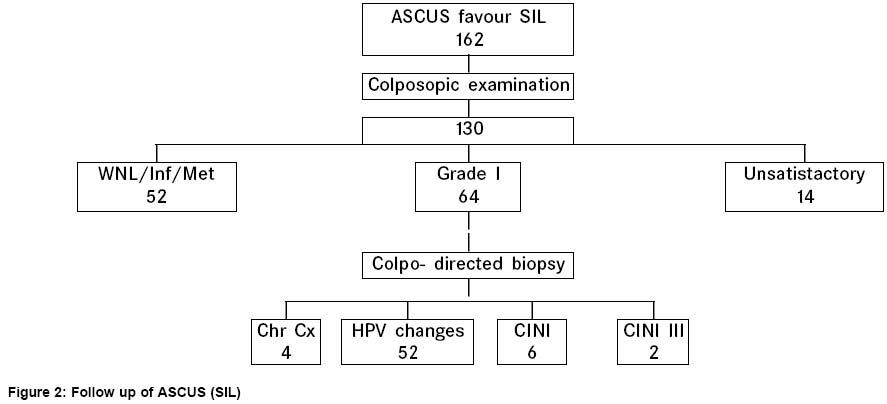
Genetics, Code Number: cn03003 ABSTRACT BACKGROUND: In Bethesda System of reporting cervico-vaginal smears, the equivocal epithelial cell abnormalities have been categorised as "atypical squamous and glandular cells of undetermined significance " (ASCUS and AGUS). These abnormalities may harbour minor lesions attributed to mere inflammatory changes to potentially serious high grade lesions. It is recommended to further qualify these lesions according to whether they favor a reactive or a neoplastic outcome. AIMS: We undertook the present study to assess the significance of ASCUS qualifiers. MATERIAL AND METHODS: A total of 12071 women were screened for early detection of cancer cervix. The women with ASCUS diagnosis were further qualified as ASCUS favor reactive and ASCUS favor SIL (Squamous intraepithelial lesion) according the Bethesda 1991 system of reporting. ASCUS-reactive cases were followed up by a repeat smear examination and persistent ASCUS cases were taken up for colposcopy and biopsy if indicated. All ASCUS-SIL cases were taken up for immediate colposcopy. RESULTS : The pick up rate of high grade lesions was not significantly different (P=0.47; Chi square test) on the follow up of ASCUS-reactive (2/222) and ASCUS-SIL (2/130) groups. The low grade lesions were picked up in 10/222 ASCUS-reactive and 58/130 in ASCUS-SIL, which was statistically significant (P <0.001). CONCLUSIONS:The results of our study indicate that it is not worthwhile to qualify these lesions as majority of ASCUS-SIL also revealed only low grade epithelial which have a benign biological behaviour. Key Words: Bethesda system, Atypical squamous cells of undetermined significance, Cervical smear. Introduction The Bethesda system of reporting cervico-vaginal smears has designated a specific term "atypical squamous cells of undetermined significance" (ASCUS) to the equivocal cytological changes on cervical smears.1 ASCUS encompasses cellular abnormalities that are more marked than can be attributed to the reactive/ inflammatory cellular changes, but qualitatively or quantitatively fall short of a definitive diagnosis of a squamous intraepithelial lesion (SIL). Their outcome may vary from an exuberant benign lesion to a potentially serious lesion. It was recommended to further qualify ASCUS lesions as favouring a low risk or a high risk outcome.2 There are several reports in literature, supporting the subclassification of ASCUS lesions in view of their differing management protocols.3,4 Many authors recommend that ASCUS favour SIL lesions should be biopsied immediately as quite a few of them have significant epithelial cell abnormalities.5 On the other hand, there are reports which say that even the low risk ASCUS category harbours a significant percentage of abnormalities on subsequent biopsies and thus needs a close follow-up.6,7 We undertook this study to evaluate the implications of ASCUS qualification on patient outcome. Material and Methods Under a hospital based cytoscreening programme for early detection of cervical cancer, a total of 12071 women in the age group of 20-60 years were screened over a period of 18 months (Sept 2000-March 2002). The study was approved by the Institute's review board and ethical clearance committee. An informed consent was taken from all the subjects. The smears were reported according to the Bethesda system of reporting cervicovaginal smears. For the purpose of this study, all the minor cellular changes in squamous epithelial cells, like enlargement of nucleus (2-3 times that of normal intermediate cells), slight increase in N/C ratio, slight nuclear membrane irregularity, minor changes in nuclear shape and chromatin pattern and atrophic atypia were put under the category of ASCUS favour reactive process. On the other hand, non classical cellular changes suggestive of human papilloma virus (HPV) cytopathic effect were diagnosed as ASCUS favour SIL. In addition, the smears falling short of definite SIL diagnosis either due to qualitative or quantitative reasons were assigned ASCUS favour SIL diagnosis. In this study, atypia in metaplastic cells was regarded as a high grade lesion. ASCUS favour reactive cases were advised a follow up smear examination after 3 months. If the diagnosis of ASCUS persisted, they were referred for colposcopy and biopsy if indicated. ASCUS favour SIL cases were taken up for immediate colposcopy and biopsy. Those with unsatisfactory colposcopy were advised a repeat colposcopy / endocervical curettage. Results Of the total smears screened, 1067 (8.8%) were placed under epithelial cell abnormalities, out of which of ASCUS was given in 720 (5.9%), low grade squamous intraepithelial lesion (LSIL) in 194 (1.6%), high grade squamous intraepithelial lesion(HSIL) in 65 (0.56%). In 44 (0.36%) cases each a diagnosis of malignancy and AGUS was given. All ASCUS lesions were qualified as to whether favouring a reactive process; 558 (77.4%) or a SIL; 162 (22.6%). The mean age of women in ASCUS- reactive group was 35.4 years while in ASCUS-SIL it was 37.2 years. Repeat smear examination was available in 222 women in ASCUS-reactive cases till the data analysis. Of these 187 were with in normal limits / benign cellular changes. Persistent ASCUS was found in 28, LSIL in 5 and HSIL and malignancy in one case each. (Figure 1) Persistent ASCUS and above cases (35) were referred for colposcopy and biopsy. On histopathology, 22/28 of the persistent ASCUS were diagnosed as chronic cervicitis / squamous metaplasia, while in 3 cases each, a diagnosis of HPV and cervical intraepithelial lesion (CIN) I was given. Biopsy of 5 LSIL cases revealed CIN I and HPV changes in 2 cases each and squamous metaplasia in 1 case. One case each of HSIL and malignancy showed CIN III and squamous cell carcinoma respectively. Of the 130/162 ASCUS-SIL cases who underwent colposcopy, 64 revealed grade l lesions which on biopsy showed HPV in 52, CIN I in 6, CIN III in 2 and chronic cervicitis in 4 cases. (Figure 2). Discussion The term "atypia" in cervical smears has been used loosely for a wide variety of lesions ranging from inflammatory to preneoplastic pathology. According to the Bethesda system, the term "atypia" should be used only for diagnostic categories designated as ASCUS and AGUS.1 Despite its use since 1988, the category ASCUS remains controversial, especially with regards to its clinical implications. There are many reports stating that ASCUS harbours a significant number of SIL (10-43%) on follow up, however, majority of these are low grade lesions.8,9 Only a few have identified significant number of HSILs on follow up of ASCUS.5 The ASCUS rates on cytology vary from 1.6 to 9 %.8 The interim guidelines from NCI workshop conclude that an ASCUS rate greater than 5% might constitute misuse of this term. Since there are variations in the populations being screened, a provisio was added that acceptable rates of ASCUS may be 2-3 times that of SIL10 In our study the ASCUS rate was 5.9% which is slightly more than the acceptable limits. This could be because in our study we took into consideration even the minor criteria for diagnosing ASCUS so as to avoid any false negatives. However, the ASCUS/SIL ratio (2.6:1) is with in acceptable limits. Thus, though the ASCUS rate in our study was high, majority (77.4%) of these favoured a reactive outcome.We were diligent in assigning SIL qualifier and only those cases which could not be given a definite LSIL/HSIL diagnosis were kept in ASCUS-SIL (22.6%). There was no significant difference (P=0.47 ) in the outcome of these two categories as far as pick up of high grade lesions is concerned (2/222 in ASCUS -reactive vs 2/130 in ASCUS-SIL). There was a significant difference (P<0.001) in the pick up of low grade lesions in the two groups. However, keeping in mind their benign biological behaviour, we could not attach much significance to these qualifiers. Our results are in agreement with ALTS triage study, the largest study on ASCUS follow up till date. They have also reported mainly low grade lesions on follow up of ASCUS.9 However, our results are in sharp contrast with Malik et al who have reported high percentage of HSIL on follow up of ASCUS.5 This may be because they put the abnormalities in metaplastic cells into ASCUS "can not exclude HSIL" category while we classified them into definitive HSIL category as far as possible. Our results are in accordance with the Bethesda 2001 recommendations where the ASCUS diagnosis has been used strictly and ASCUS -reactive group has been eliminated because of negligible detection of high grade abnormalities in this category. The diagnosis of ASCUS has been categorized as atypical squamous cells- undetermined significance (ASC-US) and atypical squamous cells- favor HSIL (ASC-HSIL) only for those cases where either due to qualitative or quantitative reasons the smear falls short for a definitive diagnosis.11 Thus to conclude we feel that it may not be worthwhile to assign qualifiers to ASCUS lesions. Since many of these cases show morphological evidence of HPV, it might be more useful to triage them with HPV DNA typing to detect high risk cases as has been recommended in certain other studies as well.9,12 References
Copyright 2003 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn03003f2.jpg] [cn03003f1.jpg] |
| |||||||||

{kind=link}
{kind=link}