 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 40, No. 1, (January - March 2003) , pp. 27-30 How We Performed Chest Wall Reconstruction: Analysis 31 Cases Tan ZB, Lamichhane N,* Thakur B,* Liu D X,** Xiao QH** Department of Surgical Oncology; *B. P. Koirala Memorial Cancer Hospital,
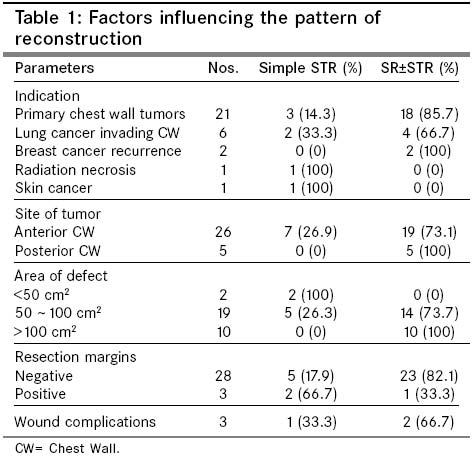
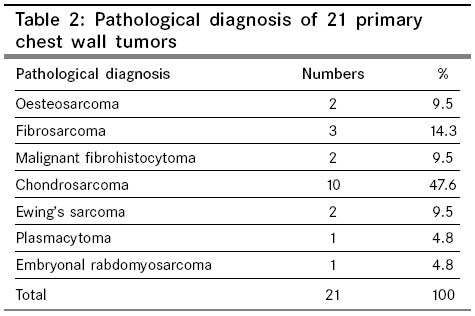
Chitwan, Nepal; and **Xingtai People's Hospital, Hebei Province, P R of China. ABSTRACT OBJECTIVE: To see the results of patients who underwent chest wall resection and reconstruction (CWRR). SETTING AND DESIGN: Retrospective descriptional study. MATERIAL AND METHODS: We retrospectively reviewed all patients who underwent CWRR at Xingtai People's Hospital in China and B.P. Koirala Memorial Cancer Hospital in Nepal. A total of 31 patients were reviewed. Among them, 20 were male and 11 female. The median age was 63 years. The indications for resection were primary chest wall tumor in 21 patients (67.7%), lung cancer with invasion of chest wall 6 (19.4%), recurrence of breast cancer 2(6.3%), radiation necrosis 1(3.2%) and skin cancer 1(3.2%). RESULTS: The mean number of rib resected was 3.6 ribs, which induced a mean defect of 97.1cm2. Concomitant resection was done in 13 patients, including lung resection 10, partial resection of diaphragm 2, and partial sternectomy 1. Seven patients underwent soft tissue reconstruction (STR) alone and 5 patients skeletal reconstruction (SR) alone. Simultaneous SR and STR were performed in 19 patients. Three patients (9.7%) developed postoperative complications. The median survival period was 22 months. CONCLUSION: Primary chest wall tumor and lung cancer invading chest wall are the most common diseases indicating CWRR. Simultaneous bony and soft tissue reconstruction was reliable for chest wall reconstruction in most cases and prevents postoperative complications. Key Words: Chest wall, Reconstruction, Tumor, Prosthesis. Introduction Reconstruction of chest wall is mandatory after its large excisions.1,2 Adequate reconstruction of chest wall prevents paradoxical movement of chest wall and overcomes deformity. There are different methods and materials used for reconstruction of chest wall in different disease conditions. According to availability of expertise and prosthetic material, approaches also differ. 1,2 In this article we have summarized 31 cases of chest wall excisions followed by reconstruction for different primary diseases in a retrospective descriptive way and tried to summarize how we are making our way of chest wall reconstruction. Material and Methods Case records of the patients those underwent chest wall excision and reconstruction at Xing Tai people's hospital (XTPH) China and B. P. Koirala memorial cancer hospital (BPKMCH) Nepal were taken for the study. Study period was from January 1998 to March 2003 at XTPH and from July 2001 to March 2003 at BPKMCH. For inclusion, there should be 1. Skeletal defect of chest wall after excision of lesion, 2. Those needed muscle-soft tissue pedicle flap and/or artificial materials for reconstruction. Those patients who only had excision of soft tissue of chest wall and those had bony defect but did not underwent reconstruction were not included in this study. Variables include age, sex, indication of excision, area of excision and defect; method of reconstruction, adjuvant therapy and immediate postoperative complications. Indication of excision is the primary disease that required chest wall excision. Area of defect is calculated as the area of bony defect that is the multiplication of length and breath of the area; if only one length is mentioned in the operation procedure note, then area of circle with that dimension as a diameter is taken. Patterns of reconstruction are 1. Simple soft tissue reconstruction (STR) i.e. only the rotation of soft tissue flap is used for reconstruction, 2. Simple skeletal reconstruction (SSR), i.e. artificial reconstruction material was used for stability of thoracic cavity, no flap is made, 3. Skeletal reconstruction and soft tissue flap reconstruction (SR+STR) where thoracic cavity is stabilized with Prosthesis and soft tissue flap. Patients from XTPH were 26 and BPKMCH 5. Males were 20 and female 11. Age ranged from 8 to 72 years with median age of 63 years. Patients had visited hospital after symptoms for 15 days to 16 months with median time of 4 month. Sites of disease were at right chest wall in 18 cases, left in 13; 11 were at anterior chest wall, 15 at lateral chest wall and 5 at posterior chest wall. Primary diseases that needed chest wall excision are listed in table 1. Among 21 primary chest wall tumors, eighteen were primarily treated for first time and 3 were recurrent diseases. For pathological details of the tumor, see table 2. In 6 cases of lung carcinoma invading chest wall, 4 were squamous cell carcinoma, 2 were adenocarcinoma. Results Resected chest wall consisted of ribs, soft tissue, muscles and sometimes skin. Numbers of resected ribs were 2 to 7, average 3.6 ribs. Area of defect was 20 to 220 cm,2 average 97.1 cm.2 Combined excision of lung was done in 10 patients, partial excision of diaphragm was done in 2 patients, and resection of lower part of sternum was done in 1 patient. Among the 10 patients in which lung was resected with tumor of chest wall; Wedge resection was done in 4 patients; lobectomy was done in 5 patients and bilobectomy in 1 patient. In 3 cases margins were positive for tumor, one at resected rib and other 2 at the soft tissue superficial to the tumor. Method of reconstruction: STR was possible in 7 (22.6%) patients. SSR was possible in 5 (16.1%) patients. SR + STR were done in 19 (61.3%) patients. Simultaneous soft tissue and skeletal reconstruction consisted of 79.2% of all cases those underwent skeletal reconstruction. Lattismus dorsi muscular flap was rotated in 20 patients, lattismus dorsi myocutaneous flap was made in 3 patients. Lattismus dorsi myocutaneous flap along with omental flap was made in 3 patients. Teflon sheet was used in 19 cases, prolene mesh in 4 patients and fascia lata in one patient to rebuild the chest wall rigidity. For factors those influenced reconstruction see table 1. Altogether 3 patients developed postoperative complications, one developed wound infection in STR case, and other 2 SR cases developed fluid collection in between Teflon sheet and overlying tissue. All of these patients became good after conservative management. Six patients taking part in this study had received neoadjuvant chemotherapy (4 lung cancer and 2 breast cancer). Adjuvant chemotherapy was given to 11 chest wall tumors, 2 breast cancer patients and 6 lung cancer patients. Radiotherapy was given to 5 chest wall tumors and 2 lung cancers. In 3 margin positive cases it was given in adjuvant setting. Other 4 patients received radiotherapy for their recurrence at local site afterwards. Follow-up study was possible in 25 cases; median survival time is 22 months. Disease free survival is 11.5 months. Discussion Chest wall excision and reconstruction is needed for the management of primary tumor of chest wall, severe infection to chest wall, radiation induced necrosis of chest wall and deep infiltrating skin cancers of the chest etc. Disease types in different reports differ according to the authors and disease he/she is treating with (See table 3).3-5 As our report is made from a department of surgical oncology of general hospital and a cancer hospital, most of our cases are cancers/tumors; 67.7% primary chest wall tumors, 19.4 % lung cancers, 6.45% recurrent breast cancers, 3.22% radiation necrosis and 3.22% skin cancer. Different disease has different patterns of chest wall destruction so area of excision and subsequent chest wall reconstruction differ. Recurrent breast cancer, radiation necrosis or local infective diseases has significant skin, soft tissue and muscle destruction so enough soft tissue reconstruction in mandatory. Primary chest wall tumors are invading through the full-thickness of chest wall and most of the time has tendency of local recurrence. So extensive excision with clear margins is mandatory that subsequently needs bone and soft tissue reconstruction.1 Resectable lung cancer when invades into chest wall has less extensive invasion through the chest wall. As it dose not involve the superficial layers of muscles, so no reconstruction is needed most of the time. Facciolo et al reported 1855 cases of nonsmall cell lung cancers (NSCLC), 104 (5.6%) among these had chest wall invasion. They did full thickness chest wall excision for all these cases. Postoperative histopathology revealed that only parietal pleura was invaded in 28 cases (26.92%), soft tissue was also involved in 36 cases (34.62%) and bone also involved in 40 cases (38.46%).6 Elia et al reported 110 NSCLC invading the chest wall, 63 (57.3%) cases underwent extra-pleural excision, 47 (42.7%) underwent entire chest wall excision. Thirty patients needed chest wall reconstruction and only 8 (26.7%) of them needed skeletal reconstruction.7 Burkhart et al reported 94 cases of NSCLC those underwent chest wall excision, 61 cases underwent chest wall reconstruction.8 Walsh et al reported 51 sarcomas of the chest wall, 34 of them needed prosthesis reconstruction and 24 were repaired with muscle flaps.9 In our study, 18 (85.7%) of 21 chest wall tumors needed skeletal and/ or soft tissue reconstruction and soft tissue reconstruction only was enough in 3 patients. Skeletal and/or soft tissue reconstruction was done in 4 patients and soft tissue reconstruction was done in 2 patients among the 6 NSCLC patients. Bone reconstruction rate is higher in chest wall tumors. The decision not to reconstruct the skeleton depends on the size and location of the defect and whether the wound is infected. In general infected wounds should not be reconstructed simultaneously. Similarly defects less than 5 cm in greatest diameter anywhere on the thorax are usually not reconstructed. At anterior and lateral chest wall, muscle layer is thin and weak so whenever there is defect of largest diameter greater than 5 cm, bone reconstruction with artificial materials is mandatory and most of them may need soft tissue flap reconstruction at the same time. Likewise high posterior defects less than 10 cm in diameter do not require reconstruction because the overlying scapula provides support. However, if the defect is located near the tip of the scapula, defect even if less than 5 cm in size should be closed to avoid impingement of the tip of the scapula in to the chest wall with movement of the arm.1 In practical, as the defect after the resection of chest wall tumor may be irregular, this is why the greatest diameter of the defect may not reflect the exact area of defect. We calculated the surface area of defect and found that 2 cases with defect less than 50 cm2 were satisfactorily repaired with soft tissue reconstruction only. For those 10 patients with defect greater than 100 cm2, skeletal reconstruction was needed. It suggests that surface area of the defect is a major factor to influence pattern of reconstruction. So all larger defects anywhere on the chest should be reconstructed and either autogenous tissue or prosthetic material may be used. Stabilization of the bony thorax is best accomplished with prosthetic materials. At XTPH, Teflon sheet was used for repair and at BPKMCH Prolene mesh was used. Both of these materials gave satisfactory rigidity to the chest wall because when these materials were kept under tension, the rigidity of prosthesis was improved in all directions. Deschamps and colleagues think Prolene mesh cannot restrict pleural fluid and air to come out into the wound that may cause to increased rate of infection.3 Fortunately our experience shows none of our 4 cases where Prolene mesh was used had the complications like chest wall emphysema or seroma. We applied compression bandage to the chest wall, did not keep a drain between the mesh and the muscular flap so that the pleural fluid and air can not come into the wound, rather the wound site transudate can enter into pleural cavity and drained through the chest tube. This is how we explain our results. Two millimeter Gore-Tex soft tissue patch and Marlex are also reported to be frequently used prosthesis but we lack the experience with these material due to unavailability. Some Chinese authors have used straps of glass fibers also to reconstruct and said infection rate is very low.2 Soft tissue reconstruction of muscle flap or omental flap along with the Prolene or Teflon increases the air tightness of the chest cavity and enhances the absorption of serous fluid. This subsequently decreases the chance of wound infection. It has got more significant role when mesh is used. We adopted soft tissue reconstruction in cases where there is no adjacent muscle to cover the wound after suturing of the prosthesis or where adjacent muscle coverage is unsatisfactory. Our combined reconstruction rate is 79.2%, which is high compared to the 50 - 60% which is frequently reported in medical literature.1-5 We consider low rate of wound complication is contribution of the simultaneous soft tissue and skeletal reconstruction. So we come into conclusion of Primary chest wall tumor and lung cancer invading chest wall are the most common diseases indicating CWRR. Simultaneous bony and soft tissue reconstruction was reliable for chest wall reconstruction in most cases and prevents postoperative complications. References
Copyright 2003 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn03004t3.jpg] [cn03004t1.jpg] [cn03004t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}