 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 40, No. 1, (January - March 2003) , pp. 31-33 Case Report Colloid Cyst of the Third Ventricle: A Cause of Sudden Death in a Child Kava MP, Tullu MS, Deshmukh CT, Shenoy A*
Departments of Pediatrics and *Pathology, Seth G. S. Medical College and KEM
Hospital, Parel,
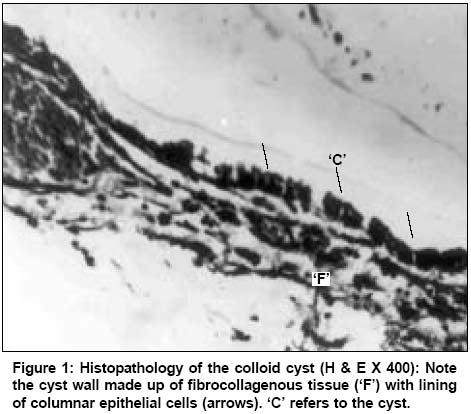
Mumbai - 400012, India. Code Number: cn03005 ABSTRACT Colloid cyst is a rare benign intracranial neoplasm, commonly located in the third ventricle. Though headache and visual symptoms are classical, the patients may present with sudden neurological deterioration. We present a ten-year-old male child who presented with sudden neurological deterioration due to colloid cyst of the third ventricle resulting in death. The child had intermittent headache for three months, for which medical attention was not sought. This report details the case and a short review of the condition is presented (with emphasis on the clinical features and importance of early diagnosis). Management (including surgical methods and conservative treatment) of third ventricle colloid cysts is briefly reviewed. Key Words: Brain, Cerebrospinal fluid, CT scan, Headache, MRI, Stereotactic surgery, Tumor, Ventricle. Introduction Colloid cyst is a rare benign intracranial neoplasm accounting for less than 1% of intracranial neoplasms with an estimated incidence of 3.2/ million/ year.1-3 Cases of colloid cysts as well as those causing sudden neurological deterioration and death have been reported in adults.1,3 Only few such cases have been reported in children.4,5 We report a case of third ventricular colloid cyst with sudden fatal neurological deterioration. Case Report A 10-year-old male presented with frontal headache, five episodes of vomiting, three episodes of generalized tonic-clonic convulsions and altered sensorium for one day. He had history of intermittent headache since the past three months for which medical attention was not sought. Examination revealed hypothermia, tachycardia (heart rate: 120/min), hypoventilation, poor peripheral pulses and hypotension. Neurological examination revealed absence of pupillary light reflex, absence of response to pain, absence of vocalization and hypotonia. Deep tendon reflexes were depressed and superficial reflexes were absent. The child was resuscitated, given cardiorespiratory support (mechanical ventilation, dopamine and adrenaline), but sustained terminal cardiac arrest after about 36 hours. Blood counts and biochemical profile was normal. Neuroimaging study could not be performed. At autopsy, a cyst was seen in the third ventricle measuring 3 X 3 cm. The cerebrospinal fluid (CSF) was under pressure. Cerebral edema, massive hydrocephalus and petechial hemorrhages over the cortical hemispheres were noted. Histopathological study revealed colloidal cyst lined by cuboidal to columnar epithelium (Figure 1). Discussion The commonest site of occurrence of colloid cyst is the third ventricular roof posterior to foramen of Monro (size ranging from 1 to 3 cm).2,4 Rarely, the location may be lateral ventricle, septum pellucidum, fourth ventricle, cerebellum or brainstem.2 Colloid cyst is composed of fibrous capsule and an inner lining of a single layer of squamous, cubiodal or slightly columnar, ciliated or non-ciliated epithelium containing gelatinous material reacting positively to periodic acid schiff staining.2,5 If the cyst enlarges rapidly, obstruction to CSF flow occurs and raised intracranial pressure develops.5 Sudden death due to herniation of brain occurs in patients in whom CSF flow is abruptly blocked.5 Gradual enlargement permits accommodation of the enlarging mass at foramen of Monro without disruption of CSF flow and patient remains asymptomatic.5 Some cysts may stop enlarging and a steady state of CSF flow and absorption is eventually achieved.5 Colloid cysts uncommonly present in children (age of presentation being 20 to 50 years).6 The cysts may remain asymptomatic and may be incidentally detected. Though commonest presentation is with headache and often accompanied by blurred vision or vomiting, headache has been rare in some series.1 Episodes of paroxysms of headache (with change of head position), vomiting and amblyopia, or profound mental changes are classical of colloid cysts.1,3-6 The headache may not be noticed by the care takers (as in our child) or even overlooked by the physician. Gait disturbances, disturbed mentation, incontinence, dizziness, tinnitus, convulsions, diplopia and `drop attacks' may occur.1,4 Neurological findings include papilledema, hyperreflexia, Babinski sign, in-coordination, nystagmus, tremor, hyporeflexia and sixth nerve palsy.1,4 Small lesions can be asymptomatic or cause headache and cognitive impairment while large symptomatic lesions can lead to herniation and long tract signs. Although majority of patients harboring colloid cysts present with headache lasting for days to years, sudden neurological decline related to blockage of CSF flow at the level of foramen of Monro is known.5 Acute fatal neurological deterioration is known in nearly 15% cases.4,7 Literature reveals examples of failed or delayed diagnosis and sudden death; even when patients survive, they present in deteriorated damaged condition.1,3-5,7 Ryder at al reviewed patients with benign tumors of third ventricular area with sudden deterioration and death (55 of the 56 cases were colloid cysts).8 Little & MacCarty reported that 11% of patients with colloid cyst presented with sudden clinical deterioration and death.1 The occurrence of acute deterioration without warning underscores the importance of early diagnosis and treatment in this potentially curable condition.1 On neuroimaging, most cysts range from 5 to 10 mm. They are mostly hyperdense or isodense with or without contrast enhancement and ventriculomegaly.4 On T1- weighted images of MRI, most appear hyperintense and look hypointense on T2- weighted images.5 The differential diagnosis of round or oval circumscribed mass in anterior third ventricle includes aneurysms of basilar artery, hamartomas, primary or secondary neoplasms and xanthogranulomas.5 The optimum management of third ventricle colloid cysts remains unclear. Procedures like stereotactic cyst aspiration, stereotactic transcortical resection, transcallosal resection, endoscopic removal and marsupialization have been performed.2,3,5 Stereotaxic microsurgical laser craniotomy with or without biventricular shunting has been described.9 Radical removal by open or stereotaxically guided microsurgery is the method of choice since sterotaxic aspiration fails to offer a radical or permanent treatment.3,9-11 Confusion, hemiparesis, seizures, Korsakoff psychosis and rarely sudden death are known to occur post-operatively.1,4 Long-term sequel include optic atrophy, epilepsy, intellectual impairment and precocious puberty.4 Experienced centers report low post-operative complications.3,6,11 The mortality with microsurgical techniques is about 3%.3 Some workers believe that observation with close clinical monitoring and serial neuroimaging is safe in patients with incidental detection of small asymptomatic cysts and most of such patients do not require neurosurgical intervention.3,5,6 Patients with small cysts (< 1 cm) on conservative management should be informed about the possible symptoms like headache, which indicate progression of the lesion. This will help them report immediately (before neurological deterioration occurs). It has also been suggested that small lesions with solid center with wide open foramen of Monro can be observed by serial MRI studies in reliable patients, while lesions with liquid center producing anatomic compromise of the foramina need to be operated for risk of ventricular obstruction.3 Symptomatic patients and those with enlarging cysts or hydrocephalus need prompt treatment.5 Majority of patients who die suddenly have cysts size of 10 to 20 mm.3 Patients and their families should be warned of the risk of catastrophic and sudden neurological deterioration, which cannot be completely predicted by serial radiological monitoring.7 This case has been presented to increase the awareness regarding third ventricle colloid cyst, which can remain asymptomatic and be fatal with acute neurological deterioration. It should be included as a possibility in children presenting with acute neurological deterioration. Our patient had intermittent headache for three months, for which medical attention was not sought. The present case also underscores the importance of evaluation of chronic headache by appropriate neuroimaging. Colloid cyst is a favorable space-occupying lesion of the brain for successful surgical removal (because an exact pre-operative diagnosis is possible) and mortality and morbidity in these cases is unacceptable in the current era.11 Acknowledgements The authors thank Dr. N. A. Kshirsagar Dean, Seth G. S. Medical College & K.E.M. Hospital for granting permission to publish this article. References
Copyright 2003 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn03005f1.jpg] |
| |||||||||

{kind=link}