 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 40, No. 1, (January - March 2003) , pp. 34-36 Case Report Mucoepidermoid Carcinoma of the Bronchus: Is Conservative Surgery Always Justified? Menon P, Singh M, Rao KLN,* Gulati M, Saxena AK, Gupta K, Kakkar N, Vasishta RK
Departments of *Pediatric Surgery, Pediatrics, Radiodiagnosis and Histopathology,
Post Graduate Institute of Medical Education and Research, Chandigarh - 160012,
India.
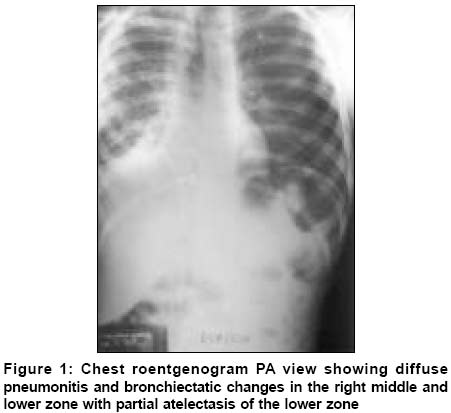
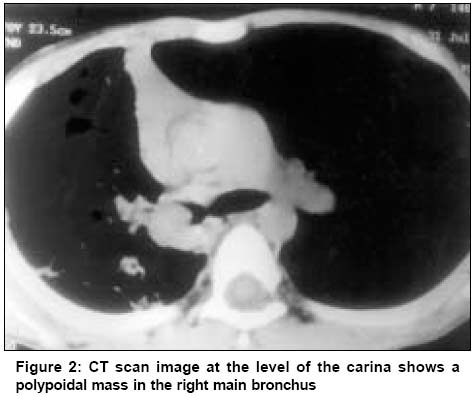
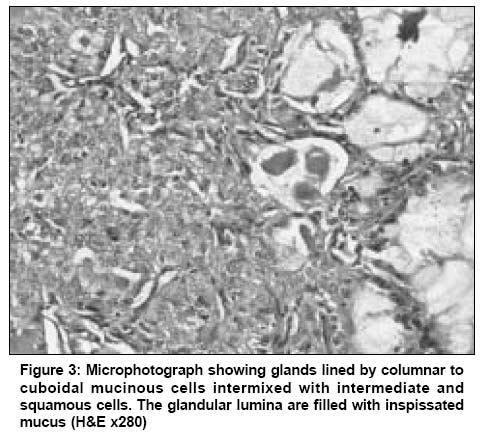
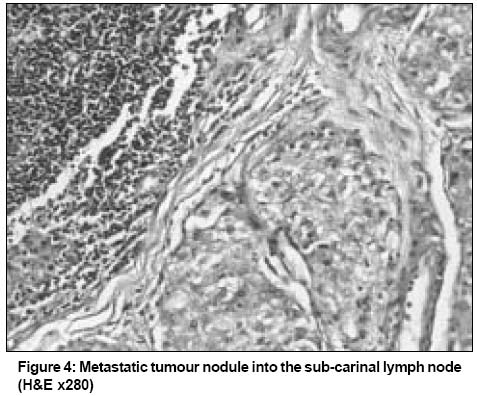
Code Number: cn03006 ABSTRACT A case of mucoepidermoid carcinoma of the bronchus in a 7-year-old boy is reported. The patient underwent right pneumonectomy. Histologically, the tumor was a low-grade muco-epidermoid carcinoma arising from the bronchus with lymph node metastasis in the drainage area. Presence of lymph node metastasis in this low-grade tumor suggests the possibility of early progression of disease in what has until now been considered a very slow growing tumor. Aggressive surgery may be necessary in these situations. Key Words: Childhood lung tumors, Bronchial neoplasm, Mucoepidermoid carcinoma, Bronchial adenoma. Introduction We report a rare case of mucoepidermoid tumor of the main bronchus with lymph node metastasis. There is no previous report of a low-grade bronchial mucoepidermoid tumor with metastasis to the lymph nodes. A search of the literature revealed a preference for sleeve resection of the bronchus in many cases. However, conservative surgical management in all the cases of mucoepidermoid carcinoma is probably not justified, especially in the presence of obvious lymph node metastasis. Case Report A 7-year-old boy was admitted with cough, expectoration of 1-year duration, associated with fever, breathlessness, loss of weight and appetite. There was one episode of hemoptysis. There was no history suggestive of foreign body aspiration or contact with tuberculosis. On examination, he was ill built with pallor, clubbing of fingers and dyspnoea at rest. There were coarse crepitations with decreased air entry on the right side of the chest. The rest of the physical examination was unremarkable. The chest roentgenogram showed atelectasis of the right lower lobe with bronchiectatic changes in the remainder (Figure 1). The sputum and gastric lavage for AFB were negative. The ESR was 28 mm in the 1st hour. Bronchoscopy showed a glistening grayish-white tumor completely occluding the right main stem bronchus starting from just below the carina. A chest computed tomography (CT) scan showed an extensive right endobronchial lesion (Figure 2) with distal post-obstructive pneumonitis, bronchiectatic changes and mediastinal lymphadenopathy. Right thoracotomy revealed a partially inflated upper lobe and the rest of the lung collapsed and consolidated with severe fibrotic changes. A sleeve resection of the bronchus was initially contemplated. However the tumor appeared to not only fill the entire length of the main bronchus expanding it thereby but had also transgressed the walls of the bronchus. Prominent lymph nodes were seen over the carina, sub-carinal and para-aortic area. The bronchus was transected at the upper extent of the tumour, which was at the carina. This revealed a polypoidal tumor projecting into the lumen of the right main bronchus. The transected edge of the bronchus at the carina was free of tumour on frozen section. However in view of the severe fibrotic changes in the lung parenchyma, extensive involvement of the entire right main bronchus and enlarged lymph nodes, plans for sleeve resection were abandoned and a right pneumonectomy with removal of all prominent lymph nodes was performed. The macroscopic examination confirmed the gross operative findings of tumor and pulmonary parenchymal pathology. The histopathological examination showed a tumor infiltrating the full thickness of the bronchus with no involvement of the adjacent lung parenchyma. It had a predominant glandular and intermediate cell component with small foci of squamous cells (Figure 3). The tumor did not show increased mitotic activity, pleomorphism or necrosis and was diagnosed as a low-grade mucoepidermoid carcinoma. The sub-carinal lymph node showed tumor tissue (Figure 4). At 1-year follow-up the child is doing well and is asymptomatic except for dyspnoea on severe exertion. Discussion Primary pulmonary or endobronchial tumors are uncommon in childhood. In a review of 383 primary childhood pulmonary tumors, 10% were mucoepidermoid carcinomas.1 Until 2001, only 52 cases of mucoepidermoid tumors had been reported in children.2 There are no known etiological factors predisposing infants and children to this tumor.1 Mucoepidermoid tumors usually arise as polypoid endo-bronchial growths in the proximal bronchi but may also involve the trachea.3 They range in size from several millimeters upto 6 cm. The grading of these tumors is based on the relative epidermoid and secretory components, the former being a minor component of low-grade tumors. The high-grade tumors also show nuclear pleomorphism, increased mitotic rate and necrosis. Low-grade tumors are mostly endobronchial, while high-grade tumors tend to involve the adjacent lung parenchyma.4 Mucoepidermoid tumors in children usually have low-grade malignant potential, remaining localized for long periods.5 Follow-up ranging upto 23 years have not shown recurrence.6 Although rare, a low-grade tumor exhibiting high-grade biologic behavior with hematogenous dissemination to skin, subcutaneous tissue and bone has been reported in an adult patient.7 Our patient, who had a low-grade variant, showed lymph node metastasis. This has not been reported earlier, except in one patient with a high-grade variant of mucoepidermoid carcinoma.8 With time, low-grade tumors may progress to high-grade malignancy, hence the need for early diagnosis and surgical excision.8 Symptoms are frequently due to bronchial obstruction with persistent cough, dyspnoea, hemoptysis, wheezing and recurrent pneumonia. Most cases often present with a long history of multiple antibiotic courses including empirical anti-tuberculosis treatment. The chest radiographs are usually abnormal showing lobar infiltrates, atelectasis or bronchiectasis. Foreign body aspiration, bronchiectasis and tuberculosis present similarly, hence the need for early bronchoscopic evaluation.5 This usually shows a partial or complete occlusion of the main stem bronchus by a lobulated gray, tan or pink mass which is firm to touch but bleeds readily. While performing bronchoscopy, awareness of superadded infection over an endo-bronchial growth is important.9 The treatment of these tumors is surgical extirpation, the exact modality depending on the site and extent of the growth. Where clear margins are obtained, sleeve resection of the bronchus is the operation of choice. However, complete resection is essential, as low-grade tumors have been known to recur locally.10 With delay in diagnosis, irreversible changes in the lung parenchyma can occur, requiring lobectomy or even pneumonectomy. Pre-operative chest physiotherapy, antibiotics and bronchial suctioning can improve the chances of preservation of the lung. Resectional and not conservative surgery was performed in our patient because of the bronchiectatic lung, inadequate free bronchial margins to attempt re-anastomosis and apparent involvement of lymph nodes. Radiotherapy and chemotherapy have been used in unresectable high-grade tumors in adults but have not been found to be very effective.4-6,10 The most common cause of delay in diagnosis is the failure on the part of the physician to suspect the diagnosis.11 Awareness of this rare but important condition while managing children with chronic respiratory symptoms is essential for proper and timely management. References
Copyright 2003 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn03006f3.jpg] [cn03006f1.jpg] [cn03006f2.jpg] [cn03006f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}