
|
Indian Journal of Cancer
Medknow Publications on behalf of Indian Cancer Society
ISSN: 0019-509X EISSN: 1998-4774
Vol. 40, Num. 1, 2003, pp. 37-38
|
Indian Journal of Cancer, Vol. 40, No. 1, (January - March 2003) , pp.
37-38
Letter to Editor
Carcinoma of Esophagus with Unusual Metastasis to Gingiva and
Phalanx
Dimri Kislay, Rastogi Neeraj, Lal Punita
Department of Radiotherapy, Sanjay Gandhi Post Graduate Institute of Medical
Sciences, Rae Bareli Road, Lucknow - 26014, India.
Correspondence to: Dr. Neeraj Rastogi. E-mail: nrastogi@sgpgi.ac.in
Code Number: cn03007
Sir,
A 60-year-old male with history of chronic tobacco chewing presented with progressive
dysphagia of 5 months duration. Endoscopy revealed a non-negotiable growth
starting at 30cms and histopathology showed squamous cell carcinoma. CT scans
showed a circumferential lower-thirds esophageal growth, which was approximately
6cms long and without extra-esophageal spread or significant regional lymphadenopathy.
The patient underwent transhiatal-esophagectomy. Operative and histopathologic
findings revealed a 6cms long growth in the lower-third of esophagus with
transmural extension. There was a satellite nodule in the middle esophagus
and enlarged paracardiac lymph nodes, which were also positive for malignancy.
In view of poor prognostic factors such as transmural extension and lymph
node positivity, the patient was given post-operative external radiotherapy
to a dose of 50.4Gy in 28 fractions at 1.8Gy per fraction by telecobalt.
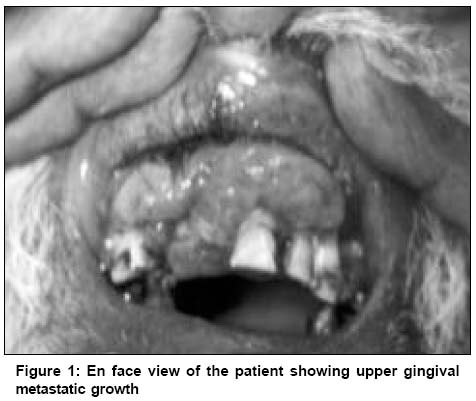
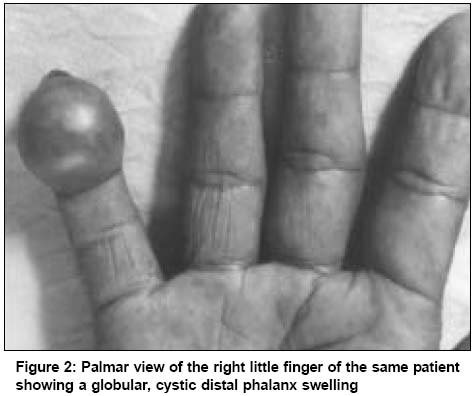
Two months following completion of radiotherapy, the patient presented with
swellings in the upper gingiva and terminal phalanx of the little finger
of right hand. The upper gingival swelling was firm, non tender and measured
4 x 2cms (Figure 1), while the swelling in the right little finger was soft,
cystic 1.5 x 1.5cms in size (Figure 2). FNAC from both sites revealed squamous
cell carcinoma. These 2 lesions were considered metastatic as they appeared
simultaneously and were reported as squamous cell carcinoma on FNAC. For
the same reason, the gingival lesion was not considered a second primary
in the oral cavity. A subsequent metastatic work up did not reveal any other
site of metastases. The patient was planned for palliative chemotherapy and
radiotherapy to metastatic sites but they could not be given as the condition
started deteriorating because of poor intake due to gingival tumor and he
succumbed to disease within 1 month of diagnosis of metastasis.
Metastatic tumors to the oral region are uncommon and mostly
located in the mandible, while only few are in the soft tissue of the oral
cavity. Review of literature has revealed only 63 cases of gingival soft tissue
metastasis with commonly encountered primary sites being lung, liver and kidney,
of which lung was the commonest.2 The prognosis of such cases is
poor, as the disease has generally disseminated by the time gingival
metastases are diagnosed. The median survival in these patients is quite dismal
and it usually ranges from 2
to 3 months.2 Esophageal carcinoma metastasizing to gingiva is uncommon
and has been reported only
once in the literature.3 Metastases to the digits of hand commonly
arise from cancer of the lung,
genito-urinary tract and breast.4 So far, only 2 cases of metastasis
to the phalanx or digital pulp from an esophageal
primary have been described.4,5 Radiological evidence of bone involvement
of the respective digit is either initially present or subsequently develops
in approximately 90%
of patients. These patients have a poor prognosis,
with survival following the diagnosis of digital
metastasis being only a few months.4
In conclusion, primary esophageal carcinoma metastasizing
simultaneously to distal phalanx of hand and upper gingiva as reported here
is an extremely rare presentation and is generally associated with a poor outcome.
Dimri Kislay, Rastogi Neeraj, Lal Punita
Department of Radiotherapy, Sanjay Gandhi Post Graduate Institute of Medical
Sciences, Rae Bareli Road, Lucknow
- 26014, India.
Correspondence to: Dr. Neeraj Rastogi. E-mail: nrastogi@sgpgi.ac.in
References
- Aisner J, Forastiere A, Aroney R. Patterns of recurrence
for cancer of lung and esophagus. In: Wittes RE, editor. Cancer treatment
symposia: Proceedings of the workshop on patterns of failure after cancer
treatment.
Washington DC: US Department of Health and Human Services; 1983. Vol 2.
pp. 87.
- Shimizu T, Nishimura T, Kaneko M, Morita T, Mizuno A, Sugiyama
A. Metastatic tumours of the gingiva- report of 3 cases. Gan No Rinsho
1990;36:719-27.
- Ide F, Shimoyama T, Haga H, Horie N. Basaloid squamous
cell carcinoma of the esophagus metastatic to the gingiva: a case report.
Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997;83:584-7.
- Houston JD, Telepak RJ. An isolated digital metastasis
of esophageal basaloid squamous cell carcinoma. Clin Nucl Med 2000;25:557-8.
- Silfen R, Amir A, Tobar A, Hauben DJ. The digital pulp
as a presenting site of metastatic esophageal carcinoma. Ann Plast Surg
2001;46:183-4.
Copyright 2003 - Indian Journal of Cancer
The following images related to this document are available:
Photo images
[cn03007f1.jpg]
[cn03007f2.jpg]
|

{kind=link}
{kind=link}