 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 40, No. 2, (April - June 2003) , pp. 71-76 Haematologic and Immunophenotypic Profile of Acute Myeloid Leukemia: An Experience of Tata Memorial Hospital Ghosh S, Shinde SC, Kumaran GS, Sapre RS, Dhond SR, Badrinath Y, Ansari R, Kumar A, Mahadik S, Chougule AB, Nair CN
Haematopathology, Laboratory, Department of Medical Oncology, Tata Memorial Hospital,
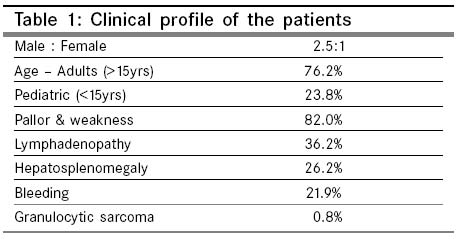
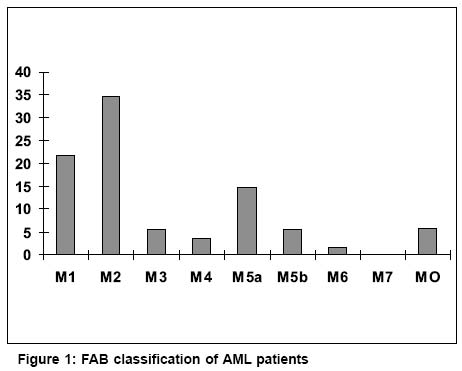
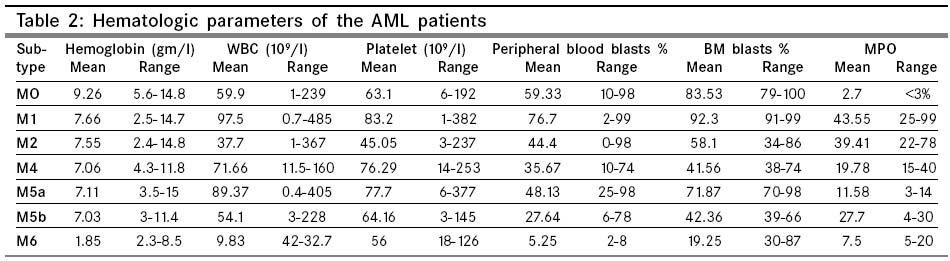
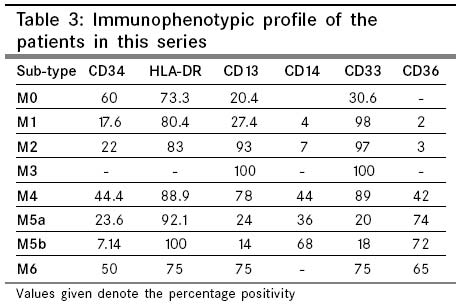
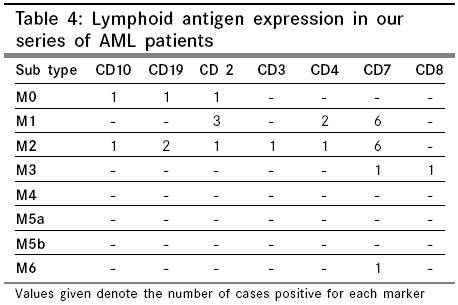
Mumbai, India. Code Number: cn03011 ABSTRACT OBJECTIVES: To study the hematologic and immunophenotypic profile of 260 cases of acute myeloid leukemia at diagnosis. MATERIAL AND METHODS: This is a retrospective analysis of 260 cases of AML diagnosed at our institution between 1998 and 2000. Diagnosis was based on peripheral blood and bone marrow examination for morphology cytochemistry and immunophenotypic studies. SPSS software package, version 10, was used for statistical analysis. RESULTS: Seventy-six percent of our cases were adults. The age of the patients ranged from one year to 78 years with a median age of 27.2 years. There were 187 males and 73 females. The commonest FAB subtype, in both children and adults, was AML-M2. The highest WBC counts were seen in AML-M1 and the lowest in AML-M3 (10-97x109/L, mean 53.8x109/L). The mean values and range for hemoglobin was 6.8gm/l (1.8gm/l to 9.2gm/l), platelet count 63.3x109/L (32_83x109/L), peripheral blood blasts 41.4% (5 to 77%) and bone marrow blasts 57.6% (34 _ 96%). Myeloperoxidase positivity was highest in the M1, M2 and M3 subtypes. CD13 and CD33 were the most useful markers in the diagnosis of AML. CD14 and CD36 were most often seen in monocytic (38%) and myelomonocytic (44%) leukemias. Lymphoid antigen expression was seen in 15% of cases. CD7 expression was the commonest (11%). CONCLUSION: AML accounted for 39.8% of all acute leukemias at this institution. The most common subtype was AML-M2. Myeloperoxidase stain was a useful tool in the diagnosis of myeloid leukemias. CD13 and CD33 were the most diagnostic myeloid markers. Key Words: Acute myeloid leukemia , Incidence, FAB, Morphology, Immunophenotype. Introduction Acute myeloid leukemia (AML) is a group of neoplastic disorders characterised by the proliferation and accumulation of immature hematopoietic cells in the bone marrow and blood. AML accounts for approximately 20% of acute leukemia in children and 80% of acute leukemia in adults.1 The incidence of AML progressively increases with age and in adults over the age of 65 years, the incidence is approximately 30 times the incidence of AML in children.2 Geographic variations in the incidence and subtype of AML have been reported. The highest incidence of AML in adults is in N. America, Western Europe and Oceania and the lowest in Asia and Latin America. The highest rate of childhood AML is in Asia and the lowest in N.America and India.3 Over the last decade, immunophenotyping has become extremely important not only in determining the lineage of the acute leukemias but also in the detection of the lineage infidelity, mixed lineage leukemias and minimal residual disease. It is also suggested to have prognostic significance. Genotypic and /or karyotypic studies on AML has provided insights into the biology and molecular basis of AML that has improved the understanding of the disease as well as help develop newer treatment strategies. The cure rates for AML however, have improved only modestly over the past two decades In this study, we reviewed 260 cases of de novo AML in relation to the incidence, morphology, cytochemistry and immunophenotype at diagnosis. Material and Methods A total of 851 cases of de novo AML were diagnosed at this institution over a period of three years between 1998 and 2000. However only 260 cases were analysed for the study as the diagnostic workup was complete in these cases. Clinical details were obtained by going through the cases records. Sixty-two patients belonged to the pediatric age group while there were 198 adults. There were 187 males and 73 females. All patients were diagnosed on the basis of peripheral blood counts, peripheral smear examination, bone marrow aspiration, cytochemistry and immunophenotyping by flow cytometry. Wright stained bone marrow aspiration smears were examined and classified into one of eight AML subtypes. Myeloperoxidase (MPO) stain was done in all cases and non-specific esterase wherever indicated. Immunophenotyping was done by flow cytochemistry on Ficoll-Hypaque separated mononuclear cells from heparinised bone marrow aspirates or peripheral blood.4 Commercially available monoclonal antibodies were obtained from BD, Pharmingen, Dako. The panel of antibodies was as follows: CD34, HLA-DR, CD13, CD14, CD33, CD36, CD19, CD10, CD2, CD3, CD4, CD7, CD8. Immunostaining of at least 20% of the cells was required for a surface marker to be considered positive. Coexpression of the surface markers was analysed when antibodies of more than one lineage were present. Statistical analysis was performed by the SPSS software package, version 10. Results Out of a total of 2138 cases of acute leukemia diagnosed at this institution over a three-year period, there were 851 cases (39.8%) of acute myeloid leukemia. In our series of 260 patients, 62 patients (23.8%) were less than fifteen years while there were 192 adults (76.2%). Clinical Features There were 187 males and 73 females with a male to female ratio of 2.5:1. The majority of our patients (82%) presented with pallor and weakness. Lymphadenopathy was fairly common and seen in 94 patients (36.2%). Cervical lymph nodes were most often involved followed by the axillary nodes. Hepatosplenomegaly was seen in 68 patients (26.2%). Bleeding was present in 57 patients (21.9%). It was most common in the AML-M3 and M5b categories and seen in the mucosa and skin. Two patients with acute myelomonocytic leukemia presented with extramedullary leukemia. Both these patients presented with orbital masses and belonged to the pediatric age group (Table 1). FAB Subtype (Figure 1) The commonest FAB subtype in adults in our series was AML-M2 at 32% followed by the monocytic leukemias (20%). AML-M1 accounted for 16% of all adult AML. AML-M6 was less common subtype at 1.6%. There was no case of AML-M7 in our series. In the pediatric age group the distribution of the AML subtypes was similar to that seen in the adults. The AML-M2 subtype was most frequent (42%) followed by the AML-M5 (20%) and M1 (16%) categories. The frequency of AML-M3 varied between 5-6% in both the pediatric and adult age groups. Laboratory parameters The WBC count was highest in case of AML-M1 with a mean of 97x109/L followed by the AML-M4 and M5 subtypes (80-90 x109/L). The lowest WBC counts were observed in the AML-M3 category at 10 x109/L. The percentage of blasts in the peripheral blood was highest in the M1 FAB subtype, that is 47%. The bone marrow blast percentage was least in the AML-M4 subtype (42%). Myeloperoxidase staining was considered positive when at least three percent of the leukemic blasts took up the stain. In case of AML-M3, the abnormal promyelocytes showed intense MPO positivity. The myeloblasts in AML-M1 and M2 also showed strong MPO staining. The hemoglobin levels ranged from 4.8gm/dl to 9.3gm/dl. Platelet counts varied between 32.8 x109/L to 83 x 109/L. (Table 2) Immunophenotyping The positivity of the stem cell marker CD34 was in the range of 18.5% to 66.7% among the various subtypes. The highest positivity was seen in the M0 and M6 FAB subtypes. HLA-DR positivity was highest in case of AML-M2 and was less in the M0 and M4 subtypes. CD33 was the myeloid marker that was most commonly present in all the AML subtypes. CD34 and HLA-DR expression was absent in all cases of promyelocytic leukemias. It was positive in all cases of M0, M1, M3, M5b and M6 categories. CD13 was the next most commonly expressed antigen showing 100% positivity in the M3, M4 and M6 categories and ranging from 80-90% in the other subtypes. CD14 and CD36 positivity was more commonly associated with the monocytic leukemias. CD14 expression ranged between 3.7% to 44.4% and the highest was seen in the M4 subtype. CD36 expression was highest in the M5a, and less in AML-M5b and M4 categories. CD14 and CD36 were negative in all cases of AML-M3. (Table 3) In our study, expression of lymphoid antigens was seen in 15% cases of AML. CD7 was the most commonly expressed lymphoid antigen (11%) and CD10 expression was least often seen (0.8%) (Table 4). Discussion Acute myeloid leukemias are a group of heterogenous disorders with respect to morphologic, immunophenotypic and cytogenetic features. Approximately 9200 cases of AML are diagnosed in the US each year.3 in adults, AMLs account for 80-90% of all acute leukemias. In contrast to the high frequency of AML in adults, the annual incidence of AML in children is low and accounts for 5.6 per million population.5 In our series, adult AML accounted for 76% of all acute leukemias and childhood AML stood at 24%. In India, the Mumbai Cancer Registry has recorded an incidence of 3.3/ million populations in the age group from birth to 19 years. Kuwait and India have the lowest incidence of childhood leukemia.5,6 The incidence in case of adult leukemia is lower in Asia and Latin America compared to N. America, West Europe and Oceania.7 Most studies have found a higher incidence of AML in males although the male predominance is not as distinct as in ALL. In our series, a male preponderance was present, with a male to female ratio of 2.5:1. Several known congenital and other risk factors have been identified in the etiopathogenesis of AML.1-5,8 Exposure to high dose radiation, occupational exposure to benzene and prior chemotherapy, inherited genetic disorders such as Downs syndrome, Bloom syndrome, Fanconis anemia and neurofibromatosis are some of the known risk factors.1,5 However the vast majority of patients have no known predisposing factor. Subtypes The commonest AML subtype in our series was AML-M2 at 34% which is slightly higher than frequency of 27-29% reported in the literature.1,3,9 Advani et al has also observed a higher frequency of AML-M2 in both pediatric and adult population from the same institution.10,11 The proportion of AML-M4 in our series was 3.5%. This is much less compared to the 16-25% reported in the literature.1,3,9,12 Roberts et al have reported a frequency of 40% in case of AML-M4.12 The incidence of APML in our study was 5.4% and conformed to the reported frequency in the literature at 5-10%. AML- M5a and M5b together constituted 20% of our patients, higher than the reported frequency of 2-9%. Incidence of AML-M6 was 1.6%, less than 3-5% quoted in the literature. In the pediatric age group, the AML-M2 was the most frequent subtype followed by the monocytic and myelomonocytic leukemias, AML-M4 and M5. There was no case of AML-M7 in our series. Clinical symptoms The majority of our patients presented with pallor and fatigue. Bleeding, both mucosal and cutaneous, was most commonly seen in the promyelocytic and the monocytic leukemias. Although lymphadenopathy is not often seen in AML this was present in 36% of our cases. The high incidence of lymphadenopathy has also been reported by Advani et al from the same institution.8 Hoffman has reported the presence of splenomegaly in 50% of his cases. In our series, however, splenomegaly was seen in 26% of patients. Extramedullary myeloid sarcoma was seen in two pediatric patients. Granulocytic sarcomas are more common in children than in adults and most commonly involve the eye and /or periorbital tissues. Geographic variations have been reported in the distribution of extramedullary leukemia and are more frequently reported from the African countries such as Uganda, Egypt and Turkey. Shome et al have reported an incidence of 17.9% for orbital granulosarcoma occurring in patients with ANLL.13 It is commonly associated with the AML-M4 subtype which was also the subtype in our patients. Granulocytic sarcomas have also been observed in the AML-M2 subtype with t(8;21) and leucocytosis.3 However extramedullary leukemia is reported to adversely affect the hematologic remission rate and overall survival in patients with t(8;21).14 Immunophenotyping Immunophenotyping has become an important diagnostic tool in establishing the diagnosis and classification of acute leukemias. It is useful in the early detection of minimal residual disease and is also reported to have prognostic value. Early myeloblasts express CD34 and HLA-DR but these are lost by the promyelocyte stage.15 Twenty five percent of our cases were CD34 positive and the highest positivity was seen in the M1 and M2 subtypes. Borowitz et al have reported a higher positivity of CD34 (45%) in the more immature leukemias and a strong association with loss or partial deletion of chromosome 7 and 5. Further, it has been observed that patients with CD34 positive AML were half as likely to enter complete remission as their CD34 negative counterparts.16,17 In most reports CD34 positivity has varied between 23 _ 61%. Callea et al have found a strong correlation between HLA-DR positivity and AML- M4 and M5 subtypes. The author also reports a higher percentage of complete remissions in HLA-DR negative cases as compared to the HLA-DR positive ones.18 The leukemic cells in all cases of M0 through M5 commonly express various combinations of CD13, CD33, CD65, CD117 and MPO. However, except for the monocytic markers and megakaryocyte associated markers CD41a, CD61 and CD42b antigens, other myeloid associated markers (CD11b, CD11c, CD13, CD33, CD15, CD65, CD66, CD117) are not useful in distinguishing the different subtypes of AML.15 The antigenic profiles of myeloid and monocytic leukemias may not be the same as the normal myeloid or monocytic development in that they may represent a) ansynchronous antigen expression, b) gain, loss or inappropriate density of myeloid antigen and c) aberrant expression of lymphoid antigens. The AML-M1 subtype is usually associated with expression of CD13, CD33, CD34, CD65, CD117 and HLA-DR in variable combinations. The leukemic blasts in cases of t(8;21)(q22:q22) associated AML-M2 have a distinct immunophenotype. They exhibit CD34, CD65, HLA-DR but CD33 and CD13 expression is very weak or sometimes may be absent. Many of them weakly express CD19 and less commonly CD56. Incidence of positivity for the stem cell associated antigen, CD34 and HLA-DR, in t(8;21) AML cells was significantly higher than those in other AML with granulocytic maturation such as AML-M2 without t(8;21) and AML-M3.19 The blasts of AML-M2 without the t(8;21) may also express CD34, CD65, HLA-DR. However the intensity of CD33 and CD13 antigen expression by these blasts usually exceeds that of t(8;21) positive blasts. CD19 is rarely detectable whereas T- cell associated antigen CD2 and 7 are more often noted on the blasts of AML-M2 without t(8;21).15 Cells of M3 and M3v AML strongly express CD9, CD13, CD33 and CD65 but lack CD34 and HLA-DR. Aberrant expression of CD2 is seen in 40 to 45% cases but more so in the M3v variant. Leukemic cells of a hyperbasophilic M3v AML may express CD34, HLA-DR, CD117 and rarely TdT.15 Moreover, the rare leukemias that morphologically resemble AML-M3 but have a t(11;17)(q24;q21), t(3;15)(q21;q22) or t(X;15)(p11;q22) can have antigenic profiles similar to AML with t(15;17).[11]Acute monoblastic leukemias are characterised by the expression of HLA-DR, CD11b, CD11c, CD33, CD65, CD15, CD36, sometimes CD117 and only rarely CD34. CD56 antigen expression in AML blasts is an important
adverse prognostic factor. It identifies a subset of patients with a
poorer prognosis in patients with t(8;21) and t(15;17) in the AML-M2
and M3 subtypes.20 A significant shortening of survival for
patients with at least 10% CD14 positive cells in FAB subtypes M0, M1,
M2, and M3 has been reported.21 Ball has reported an association
between lymphocyte antigen positivity and expression of hemopoietic progenitor
cell antigen CD34 and NK cell marker CD16.22 He has also identified
CD2 as a marker of
poor prognosis.22 CD65 expression is reported to be a significant
risk factor for extravascular AML infiltration.23 Lymphoid antigen
expression was seen in 15% of our cases and the highest positivity was seen in
case of CD7 at 11%. Lymphoid antigen positivity has been reported between 16-22%
and CD7 appears to be the most commonly expressed marker (28.4%).22,24,25 There
is much controversy regarding the role of lymphoid antigen expression in AML.
Most authors are now of the opinion that most cases of AML with lineage infidelity
appear to do poorly.1 There appears to be an association between expression
of lymphoid antigens and certain AML subtypes. Expression of CD2 and CD19 are
associated with AML-M3 and M2 respectively.12,17 Our study concludes that AML accounted for 39.8% of all leukemias diagnosed at our institution. Seventy six percent of these patients were adults. The commonest subtype in both children and adults was AML, M2. CD13 and CD33 were the most useful markers in the diagnosis of AML. Aberrant lymphoid expression was seen in 15% cases and CD7 was the lymphoid marker most often expressed. References
Copyright 2003 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn03011t4.jpg] [cn03011t3.jpg] [cn03011f1.jpg] [cn03011t2.jpg] [cn03011t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}