 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 40, No. 2, (April - June 2003) , pp.82-83 Letter to Editor Alveolar Soft Part Sarcoma: A Unique Tumor with Disputed Histogenesis Amit Nair, Dinker R. Pai, Jagdish S., Krishnan R.*
Department of Surgery and *Pathology, JIPMER, Pondicherry 605006, India.
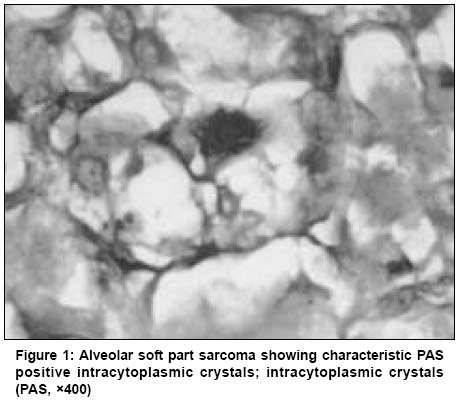
Code Number: cn03014 Sir, We wish to bring to your kind attention a case of Alveolar Soft Part Sarcoma (ASPS) managed in our institute. A 32-year-old male presented with history of rapidly increasing swelling over the left forearm of one year duration. On examination, there was a 8 × 4 cm firm mass over the extensor aspect of the left forearm, fixed to the extensor muscles, but free from the overlying skin. There were no distal neurovascular deficits. No regional lymphadenopathy was noted. Investigations revealed no evidence of metastatic disease. Fine needle aspiration performed on the mass revealed cytological features consistent with a diagnosis of rhabdomyosarcoma. At surgery, the tumor was found to be infiltrating the underlying extensor compartment. Wide local excision was done including a margin of underlying involved muscle. The resected specimen revealed a well delineated grey-white, soft, fleshy tumor of size 7 × 5 cm, with areas of haemorrhage and necrosis. The tumor was separated from the resected margins by a thin layer of fascia. Light microscopy showed a cellular tumour composed of large, polygonal to round cells arranged in an alveolar pattern, with abundant, eosinophilic granular cytoplasm and central round vesicular nuclei, with prominent nucleoli. There was a mitotic rate of 6 per ten high power fields. The periphery of the tumor showed tumor emboli within veins. The resected margins were focally involved by the tumor. PAS stain with diastase digestion revealed diastase resistant rod shaped crystals in the cytoplasm of tumour cells (Figure 1). A diagnosis of Alveolar soft part sarcoma was made. Immunohistochemistry was not performed since the H&E appearance and PAS positive crystals were sufficiently characteristic. ASPS was first described by Christophersen in 1952. It frequently occurs from 15-35 years of age, and shows a female preponderance. The most common site is over the lower extremities.1 FNA has been shown to diagnose the lesion reliably in some cases.2-4 Our case had the characteristic histopathological features of an alveolar pattern and diastase resistant PAS positive crystals making the diagnosis straightforward. Immunohistochemical examination was not required for confirmation. Renal cell carcinoma occasionally mimics ASPS, but often shows focal tubular pattern of growth and lacks the crystals. Extra adrenal paraganglioma can also simulate ASPS due to its organoid pattern, but it too lacks the characteristic crystals. There are no pathognomonic markers for ASPS to date, though recent studies have shown that the crystals are immunoreactive to a protein MCT1 (monocarboxylate transporter) and to CD 147.5 However the significance of this finding is not known. The histogenesis of this tumor is the subject of extensive research and has yielded results varying from skeletal muscle to neural origin. Till date, none of the histogenetic hypotheses have found acceptance. These tumors are usually indolent in behaviour, but have a high propensity to recur locally after excision, and to metastasize early on. The lungs, brain and bone are common sites of metastatic disease. Tumor size and site have no significant bearing on the prognosis, and tumor resectibility is the crucial prognostic marker.6 Surgical excision remains the mainstay of therapy, and adjuvant chemotherapy and radiotherapy have no definite role in its management. In the present case the tumor was found to be infiltrating adjacent muscles and showed vascular and resected margin invasion histologically. The patient made an uneventful post operative recovery and subsequently received post operative external beam radiotherapy for residual tumor. He continues to be on follow up, with no evidence of local recurrence or distant spread, till date. This case is presented to highlight the distinctive morphological features of this unusual tumor. Amit Nair, Dinker R. Pai, Jagdish S., Krishnan R.*
Department of Surgery and *Pathology, JIPMER, Pondicherry 605006, India. REFERENCES
Copyright 2003 - Indian Journal of Cancer
The following images related to this document are available:Photo images[cn03014f1.jpg] |
| |||||||||

{kind=link}