 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 40, No. 3, (July - September 2003) , pp. 101-107 Role of Chemoradiation in Advanced Cervical Cancer Singh TT, Singh IY, Sharma DT. Singh NRK* Departments of Radiotherapy and *Biostatistics, Regional Institute of Medical
Sciences, Imphal -
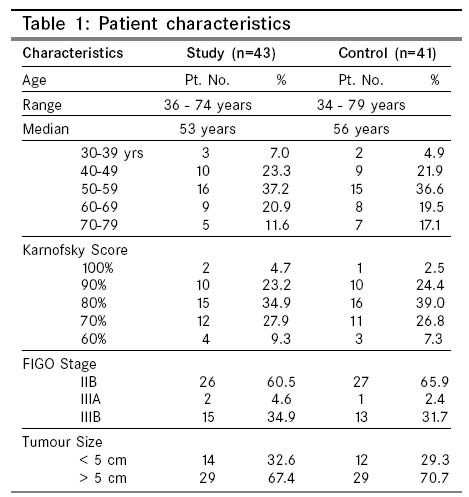
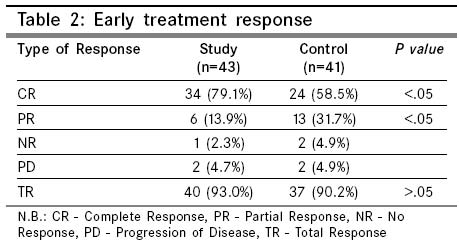
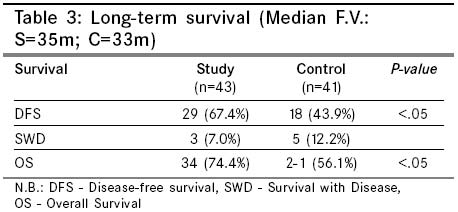
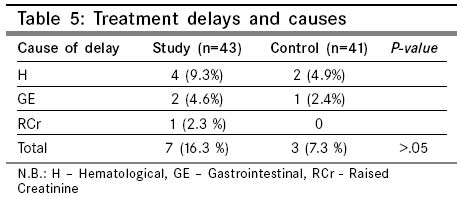
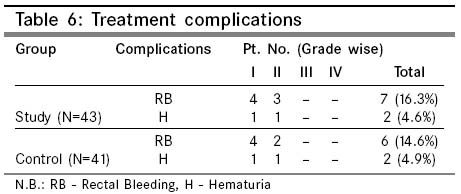
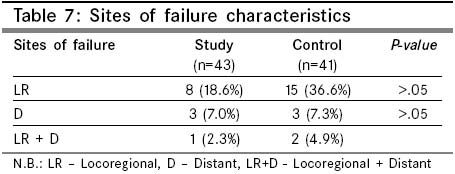
795004, Manipur State, India. Code Number: cn03016 ABSTRACT: A prospective randomized study was conducted in our department of Radiotherapy, Regional Institute of Medical Sciences, Imphal to evaluating the role of chemoradiation in the management of advanced inoperable cervical cancer (stage IIB-IIIB) taking only radiation treatment as control spanning the period 1996-1999. Of the fifty patients accumulated in the study group, three patients did not complete treatment, one expired due to other causes and three were lost to follow up. Likewise, of the forty-six patients in the control group, one patient did not complete treatment and 4 were lost to follow up. Thus only 43 and 41 patients were available for the result analysis for the study and control groups respectively. The early treatment response as assessed after two months of treatment conclusion were 79.1%, 13.9%, 93.0% and 58.5%, 31.7%, 90.2% as complete response (CR), partial response (PR), and total response (TR) respectively for the study and control groups. Our patients included in this study had a median follow up of 35 months and 33 months for study and control groups respectively. For this follow up, the disease-free survival, survival with disease and overall survival were 67.4%, 7.0%, 74.4% and 43.9%, 12.2%, 56.1% for study and control groups respectively. There was an increase in early side-effects in the chemoradiation group but the difference was not significant. Because of the early side effects, treatment delays ensued in 7 patients (16.3%) and in 3 patients (7.3%) in the study and control groups respectively. There was no significant increase in the late treatment toxicities in both the groups. Key Words: Cervical cancer, Chemoradiation, Advanced cervical cancer. Introduction Cervical cancer is the commonest tumour afflicting females in developing countries including India.1 Advanced stages of this disease is not amenable for surgical treatment. Radiation treatment is the sole definitive treatment available for this category of patients. Though cervical cancer in early stages is quite radioresponsive, for locally advanced stages, the long-term outlook has consistently remained grim for last few decades. Treatment failure outside the radiation field is well encountered, however it is the persistent / recurrent pelvic disease which remains a significant obstacle to prolonged survival.2,3 Approximately twothirds of locally advanced disease fails in treated pelvic area.3 This is because of the bulk of the primary lesion with its attendant increase in hypoxic cells, poor geometry and increase in growth fraction thereby resulting in poor radiation response. This fact is more so in developing countries where there is more tendency towards late presentation with very bulky central disease. Attempts at improving local control by increasing radiation dose are hampered by the maximum tolerated dose of surrounding organs. Innovative techniques such as hyperthermia, hyperbaric oxygen, hypoxic cell sensitizers, neutron therapy and hyperfractionated treatment schedules have all been tried but unfortunately these modalities have not demonstrated improved therapeutic response or local control. With this helplessness to improve local control and survival in the advanced stages of the disease and also being encouraged from some reports that radiosensitizing chemotherapeutic agents like Hydroxyurea, Cisplatin etc. demonstrated overall improvement of disease-free survival as compared to treatment only with radiation,4,5 we have taken up this prospective study to find out the role of chemoradiation in advanced cervical cancer. We have chosen Cisplatin as the radiosensitizing agent as it is found to be the most active agent in this tumour6,7 and has good radiosensitizing power resulting in higher progression-free survival as compared to others.8 Chemoradiation may decrease the shoulder or increase the slope of the radiation dose response curve by possible mechanisms that include direct tumour cell cytotoxicity, tumour cell synchronization, inhibition of subtotal radiation repair and hypoxic cell sensitization.9 We report here the preliminary results of our study, the median follow-up of which has attained 35 months for study group and 33 months for the control group respectively. Material and Methods This is a unicentre prospective randomized study undertaken in the department of Radiotherapy, Regional Institute of Medical Sciences, Imphal (India) spanning the period 1996-1999. Patients who are previously untreated histologically confirmed invasive squamous cell carcinoma of cervix confined to the pelvis by our work-up were taken. Adenocarcinomas and adenosquamous histopathologies were excluded from the study. The stages incorporated in the study were advanced inoperable stages of IIB to IIIB. The other required criteria are sixty per cent or above Karnofsky score, adequate hematological function (Hb%-9 gm% or above, TLC-3,000/c.mm. or above; and platelete count- 1,00,000/c.mm. or above), renal function (urea 50 mg% or less and creatinine 2 mg% or less) and adequate liver function. All patients were subjected for thorough physical examination, complete blood count, blood biochemistry including liver function test, kidney function test and serum electrolytes, x-ray chest, intravenous urography in needed patients, ultrasonography abdomen, CT scan abdomen in affordable patients and cystoscopy in stage IIIB patients. Informed written consent was taken for all the patients. External beam radiation treatment (EBRT) was delivered using a telecobalt (80 cm. SSD) machine. We used box technique treating all fields daily delivering 200 cGy per fraction, one fraction a day, and five days a week. Equal loading was given for the anteroposterior and lateral ports. The upper border of the antero-posterior field passes through the upper border of the sacro-iliac joint, laterally covers the pelvic brim with a margin of one cm. and inferiorly to cover the obturator fossa. If there is vaginal spread downwards, the lower border covers it with a margin of 2 cm. A dose of 50 Gy by EBRT was given. After a gap of 1-2 weeks after the conclusion of the EBRT, one sitting of intracavitary radiation treatment (ICRT) using Selectron remote controlled LDR / MDR system was applied giving a dose of 23-25 Gy. at point A. The dose to point B was raised upto 55-60 Gy by EBRT para boost whenever involved. The patients were randomized into two groups: We used box technique Study group In this group in addition to the radiation treatment already explained above, patients were also given concomitant Cisplatin at least half an hour before EBRT and during ICRT treatment. Cisplatin was given in the dose of 16 mg/m2 IV D 1-5 repeated at 3 weeks x 2 times during EBRT and as 40 mg/m2 during ICRT. So far fifty patients have accrued in the study group. Control group In this group only EBRT and ICRT as explained above were given without any chemotherapy. So far forty-six patients have already accumulated in this group. During the whole period of EBRT in both the groups, patients were checked-up physically twice a week to note and address untoward side effects or otherwise. The patients were also subjected to weekly CBC, chemistry profile and serum electrolytes. Chemotherapy was deferred if Hb% < 9 gm%: TLC < 3,000/c. mm. or platelet count < 1,00,000/c. mm. And were restarted upon marrow recovery. Treatment was also suspended during moderate to severe diarrhoa or dehydration. Accrual goals The initial accrual goal was to recruit fifty patients each in the study as well as control groups or a significant difference in the early and late treatment results whichever earlier. After the completion of the treatment, the patients were followed-up once monthly in the first year, two monthly in the second year and three monthly thereafter till five years. Check x-ray chest and ultrasound abdomen were done every six months but if indicated, at closer intervals. Whenever there was need, CT scan was also done. Response to treatment was assessed in accordance with WHO Miller's criteria. Calculations on long term survival were done using standard chi square test and for the same, service of a statistician who is a co-author for this paper was utilized. Early and late toxiciies were analyzed as per ECOG criteria. Results For the result analysis, only forty-three patients in the study group and fort-one patients in the control group were available. The stagewise distribution of patients were 26, 2, 15 and 27, 1, 13 for stages I1B, IIIA and IIIB respectively for study and control groups. The peak age of presentation was in the fifth decade for both the groups, the median being 53 years and 56 years for study and control groups respectively. 67.4% and 70.7% of the study and control groups presented with local disease >5 cm diameter (Table 1). The early treatment response as assessed after two months of ICRT was 79.1% as CR, 13.9% as PR, 2.3% as NR and 4.7% as PD for study and 58.5% as CR, 31.7% as PR, 4.9% as NR and 4.9% as PD for control group (Table 2). Albeit the improvement of total response in the study group as compared to that of the control group is not significant, the improvement of complete response in the study group is significant (P<.05) Patients of the study group had a median follow-up of 35 months (Range 14-54 months). With this follow-up, the overall survival rate of 74.4% (Disease-free survival being 67.4% and survival with disease being 7.0%) was achieved. Patients in the control group also attained a median follow-up of 33 months (Range 13-56) and the overall survival obtained with this was 56.1% (Disease-free being 43.9% and with disease, 12.2%) - Table 3. The difference in the overall as well as disease-free survival are significant (P<.05). Toxicities The early toxicities were mild to moderate, most of the patients could tolerate them and the most common toxicity was hematological. We analyzed early treatment toxicities in terms of hematological, gastrointestinal and raised serum creatinine only. The early toxicities in the study group were: hematological in 9 patients (20.9%) - 5 patients grade I, 3 patients grade II and 1 patient in grade III; 6 patients (13.9%) gastrointestinal - 4 in grade I and 2 in grade II and raised serum creatinine in only one patient (2.3%) - grade I. In the control group, hematological toxicities were seen in four patients (9.8%) - 3 in grade I and 1 in grade II; gastrointestinal in two patients (4.9%) - all grade I and none for raised creatinine. The difference in the different toxicities in both the groups were not significant (P>.05). Because of the early treatment toxicities, treatment delays (>3 days) were noticed in 7 patients (16.3%) in the study group - because of hematological causes in four patients, gastrointestinal causes in two and for raised creatinine in one patient. In the control group, delays were seen in three cases only (7.3%) - two for hematological and one for gastrointestinal. In none of the patients, the delay in treatment was more than ten days but we had to intervene with necessary supportive treatments like blood transfusion, antibiotics, hydration and even colony stimulating factor in very few patients. In regard to the late complications, rectal bleeding was the commonest and it was seen in 7 cases (16.3%) - grade I in 4 cases and grade II in 3 patients in the study group and in, six cases (14.6%) - grade I in 4 and grade II in 2 patients in the control group. Hematuria was seen in 2 cases - grade I in 1 case and grade II in one patient in both the groups. No fistula was noticed in both the groups. The difference in the late complications were not significant (P>.05). Sites of failure In the study group, 8 patients (18.6%) failed in the locoregional area, 3 (7.0%) failed in distant areas and 1 (2.3%) failed in locoregional plus distant regions. In the control group, 15 patients (36.6%), 3 (7.3%) and 2 (4.9%) respectively failed in locoregional, distant and locoregional plus distant areas (Table 5). Discussion It is a well-known fact that advanced stages of cervical cancer with bulky disease do fail within the irradiated field in majority of the cases. Thus it has been postulated that enhanced local control might improve disease-free survival.2,3,10,11 Towards attempts in the improvement of locoregional control, chemotherapy can be incorporated in the conventional radiation treatment course in three different ways - neoadjuvant (before), adjuvant (after) and concomitant (during). Neoadjuvant chemotherapy, though responsive to cervical tumour cannot improve on long- term survival. Four larger randomized trials containing more than hundred patients have shown that neoadjuvant chemotherapy either adversely affected local control and survival12,13 or had no different effect in overall and disease-free survival14,15 compared with standard radiotherapy alone, although it gave a significant response rate. The main reason for the poor treatment result is the delay in institution of definitive radiation treatment triggering accelerated repopulation of surviving clonogens and cross-resistance to further radiotherapy.16 Postradiation adjuvant chemotherapy is fraught upon as a component of primary treatment because the already compromised vascularity by radiation change lessens drug penetration, resulting in a poor effect of chemotherapy.16 It is thus the concomitant chemoradiation which gives the best hope for a better result, the reasons being already explained earlier. Most series have already confirmed the superiority of Cisplatin over Hydroxyurea and 5-FU.7.16,17 Another problem with the later is the added toxicity on radiation mucosities. In developing countries including India, the performance status of majority of the patients are quite low and thus we had to include patients as low as 60% Karnofsky score in both the study as well as the control groups but were more or less uniformly balanced. At the same time, majority of the patients presented with very bulky locoregional disease for their stage and it was seen that in 67.4% and 70.7%, patients presented to us with central bulk > 5 cm. for study and control groups respectively (Table 1). Though our intended gap in between EBRT and ICRT was 1-2 weeks, for problems beyond our control such as patient load to O.T. days available, general holidays etc., the mean gap in our patients turned out to be sixteen days in the study and seventeen days in the control groups respectively. In our study, in the early treatment result analysis, though the total response (93.0%) in the study group and in 90.2% in the control group is statistically not significant but the achievement of complete response (79.1% vs 58.5%) is significant (P<.05) Table 2. Abbie L, Fields et al.4 using chemoradiation with cisplatin achieved 87.3% (CR), 9.0% (PR) and 3.6% (PD) in his patients. Peter G. Rose9 also noted a statistically significant improvement in CR in patients using chemoradiation with cisplatin as compared to controls (55% vs. 20%) - P<.025. Wlong L.C. et al.18 randomized 45 patients with stage II and III cervical cancers to treatment with cisplatin 25 mg/m2 weekly and radiation or radiation therapy alone. CR were noted in 55% of the chemoradiotherapy group versus 20% in controls (P<.025). However, subsequent long-term analysis of this data failed to show a survival advantage.19 Jin-Ching Lin et al.16 using concurrent PEB chemotherapy (cisplalin, etoposide and bleomycin) achieved 97.6% CR, sustained through a median follow-up time of 30 months. However, the side-effects were significantly high which included 21.4% proctitis and 1 caecum perforation among others. Pearcey et al.20 in a phase II trial of 60 patients, using concomitant cisplatin 50 mg /m2 every 10 days during external beam radiotherapy, synchronized to be completely infused 2 hours prior to the onset of RT reported an overall pelvic control rate of 78% without a pelvic relapse after 27 months. They reported pelvic control / 3 years survival by stage as 60% / 57% for 14 stage I patients, 90% / 78% for 29 stage II patients and 64 % / 50 % for 17 stage III / IV patients. Extended field RT (40 - 45 Gy) was delivered to those patients with para-aortic node involvement. There have been controversies about the optimum timing of cisplatin administration in relation to RT treatment. However, pre-clinical data suggests enhanced tumour response by a factor of 1.7 when cisplatin was administered at least thirty minutes prior to radiation treatment.21,22 Pearcey and Maclean23 have extrapolated that in terms of tumour cell kill, cisplatin appropriately synchronized with RT would be equivalent to a ten per cent increase in radiation dose, which could theoretically improve local control. In our study, the improvement in overall and disease-free survivals in the study group (74.4% and 67.4%) is significantly better (P<.05) than that of the control group (56.1 and 43.9%) Table 3. Muderspach L.I. et al.24 in a study of the effect of twice weekly carboplatin concomitant with RT in 22 evaluable patients had 19 (86.4%) complete responders of whom 15 (68.2%) remain alive: eleven patients were alive and disease-free at last visit to a median duration of 15 months follow-up (range 4 - 43 months) and four patients remained alive with disease for a median duration of 17 months (range 3 - 55 months). There were no treatment related deaths and no grade IV toxicity. Morris M. et al.25 in a prospective randomized study compared the effect of radiotherapy to a pelvic and para-aortic field with that of pelvic radiation and concurrent chemotherapy with 5- FU and cisplatin D1-5, three weekly twice during external RT and once during ICRT in 403 women with advanced survical cancer (IIB-IVA) or stage IB or IIA with tumour size > 5 cm or involvement of pelvic nodes. The median duration of follow-up was 43 months. Estimated cumulative rates of survival at five years were 73 per cent among patients treated with RT and chemotherapy and 58 per cent among patients treated with RT alone. The difference in survival was significant (p = .004). In a recent NCI release,26 results from each of five randomized phase III trials showed an overall survival advantage for cisplatin based therapy given concurrently with radiation therapy. The study included FIGO stages of IB2 - IVA . They also noted that the risk of death from cervical cancer was decreased by 30% to 50% by concurrent chemoradiation. We attribute the following for the relatively poor result in our patients: bulky central disease, anemia, low Karnofsky score, poor nutrition and general condition, low socio-economic condition and the possibility that we could have included patients with involved para-aortic nodes (some patients could not afford CT scan) - patient related and the mean gap in between EBRT and ICRT was longer (mean 16 days) - as treatment related. In our patients, there is increase in the early toxicities in the study group but the difference is not statistically significant (P>0.5). The symptoms were mostly mild to moderate and most of the patients could tolerate them. The symptoms subsided completely within two weeks following completion of treatment. The treatment delay in the study group as a result of early toxicities as compared with that of the control group was also not significant (P>.05) and in none of the patients, the delay was more than ten days - Table 6. We also didn't have any significant difference in the long-term side effects in both the groups - Table 7. Complications like fistula or severe enteritis were not noticed in any of our patients. This may be because we haven't exceeded RT dose to beyond 7,750 cGy (Manchester equivalent) at point A. Our finding of comparable long-term toxicities in both the study and control groups is in agreement with many reports from other studies.25,27 In our patients, maximum of them failed in the locoregional area (18.6%) in the study group and in 36.6 in the control group. We could not appreciate any influence of chemoradiation on the incidence of distant metastasis. This is in agreement with other reports.1,4 But Morris M et al.25 in his study to compare the effects of only radiation treatment to pelvic and paraaortic regions with that of pelvic radiation plus concomitant chemotherapy incorporating cisplatin and 5-FU (days 1 through 5 and days 22 through 26 of radiation) found significantly higher incidences of both distant metastasis (P<.001) and locoregional recurrences (P<.001) in the radiation only treatment. Conclusion There is a significant improvement in the long-term survival (overall as well as disease-free) in the study group as compared to that of the control group. In the early treatment response, though there is no significant difference in the achievement of TR, the difference in CR is significant. There is modest increase in the early treatment toxicities in the study group but the difference is not statistically significant. The late side-effects of treatment were also comparable in both the groups. References
Copyright 2003 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn03016t3.jpg] [cn03016t1.jpg] [cn03016t4.jpg] [cn03016t7.jpg] [cn03016t6.jpg] [cn03016t2.jpg] [cn03016t5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}