 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 40, No. 3, (July - September 2003) , pp. 108-112 Stones Associated Renal Pelvic Malignancies Raghavendran M, Rastogi A, Dubey D, Chaudhary H,
Kumar A, Srivastava A, Mandhani A, Krishnani N, Department of Urology and Renal Transplantation, Sanjay Gandhi Post Graduate
Institute of
Medical Sciences, Rae Bareli Road, Lucknow - 226014, India.
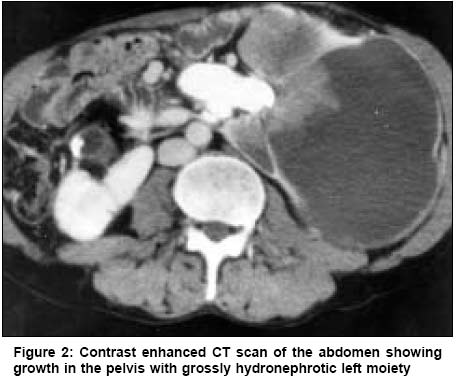
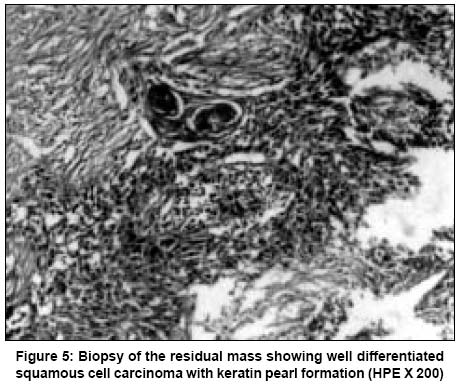
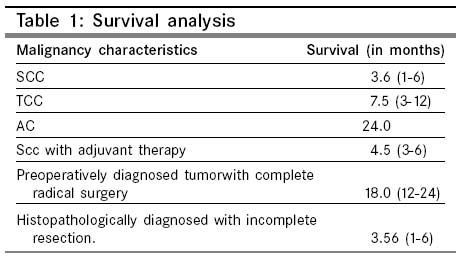
Code Number: 03017 ABSTRACT: ACKGROUND: The clinico-pathological characteristics of renal pelvic malignancies associated with stones were retrospectively analyzed. AIMS: The main objective was to define the biological behavior and prognostic factors for these malignancies. SETTINGS & DESIGN: The tumors were classified according to the pathological types. The clinical data, imaging features and pathological features were analyzed with relation to prognosis. MATERIAL AND METHODS: Eighteen cases of malignancies associated with stone disease were retrospectively studied. The institute review board permitted the study. RESULTS: High incidence (15/18) of squamous cell carcinoma (SCC) was noted. The prognosis in this group of patients was uniformly poor. The median survival time was 3.6 months in the SCC group, 7.5 months in the Transitional Cell Carcinoma (TCC) group and 24 months in the Adenocarcinoma (AC) group. Infectious and systemic symptoms were noted in the majority of the patients. Preoperative Imaging techniques revealed tumor in only 2 cases. Both underwent radical extirpation and the median survival is 18 months till date. In the other 16 patients, where the initial diagnosis was made only on histological analysis of incomplete nephrectomy specimens, the survival was 3.56 months. All patients had prolonged history of staghorn stone disease with associated non-functioning kidney. We found that the main prognostic factor was the stage of the disease. CONCLUSIONS: Malignancies associated with stone disease have insidious onset of clinical symptoms and need a high degree of suspicion to identify them pre-operatively. The grave prognosis associated with incomplete excision makes it imperative to diagnose them earlier. Key Words: Contrast enhanced CT, Radical Nephrectomy, Squamous cell carcinoma, Adenocarcinoma, Transitional cell carcinoma. Introduction Squamous cell carcinoma (SCC) and adenocarcinoma (AC) of the renal pelvis are highly uncommon tumors and constitute less than 1% of upper urinary tract neoplasms.1 With advances in modern medicine, extracorporeal shock wave lithotripsy and per cutaneous nephrolithotomy have become the treatments of choice for all cases of renal calculus disease.2 These need routine work up by means of intravenous urography and ultrasound. SCC and AC are known to be associated with chronic renal calculi and infection. Their pathogenesis is well documented. The process is assumed to begin with urothelial metaplacia due to chronic irritation and this leads to de-differentiation and finally SCC or AC. The dismal prognosis associated with these renal pelvic malignancies caused by calculus disease, urged us to study the biological behavior of these tumors. We planned to study the clinico-pathological data and imaging findings in our patients in order to find the most important prognostic features associated with these tumors. We believed that earlier diagnosis and correct prognostication will go a long way in achieving better outcomes in this group of patients. Material and Methods The department of Urology, Sanjay Gandhi Postgraduate Institute for Medical Sciences, Lucknow undertook this study. All cases of renal pelvic malignancies associated with stone disease treated in the department over a ten-year period (1992-2002) were analyzed. A database of renal malignancies is being maintained in the department. From this database, those with diagnosis of renal pelvic malignancies were extracted. Amongst these, only those associated with stone disease were included for the study. During this period 18 such patients (Mean age-61.5 years, [range: 40-82]) were found. Case records were retrospectively reviewed and specific attention was focused on the clinical features, imaging characteristics, histopathological reports and patient's survival. The clinical data included age, sex, presenting symptoms and signs, treatment modalities and the survival time. The duration of stone disease was noted. Presenting clinical features were noted. Presence of flank pain, pyuria, fever and leukocytosis were taken as signs of infectious disease. Imaging findings included Plain X-Ray, Intravenous urography, Ultrasound and CT scan (in the later part of the study). Two members of the surgical team (DD, AK) preserved the old imaging records. On intravenous urography, the function of the moiety containing the stone was noted. The CT findings included the location, maximal diameter and stage of the tumor. Associated findings were also recorded. The available operation notes and pathological specimens confirmed these. Details of surgical management were noted from the surgeon's operative description. Most of the patients were treated by simple nephrectomy, except two patients who were treated by radical nephrectomy. Survival time was counted from hospital discharge to the death of the patients. All the histopathology reports originated from the department of Pathology. Two pathologists (AR, NK) retrospectively reviewed the available histological material. The pathological type, the grade or differentiation of the tumor, the presence of lymphovascular invasion and the extent of tumor into renal parenchyma and peripelvic fat were noted. Adjuvant therapy was given to some patients after explaining fully the response rates and prognosis. The type of therapy was noted and the response to the same was also noted in order to see any survival benefit. Results Thirteen patients were men and 5 were women. The left side and right side were involved in 12 & 6 patients respectively. All patients had existing stone disease for variable duration- 8.8 years (6-11.6). Pain was the predominant presenting feature, occurring in seventeen patients. Six (6) patients also had haematuria. All patients had normal renal function and a large staghorn calculus with a non-visualized kidney on an intravenous urogram on the affected side (Figure 1). All patients also underwent pre-operative ultrasonography. Preoperative imaging picked up renal pelvic tumors in 2 out of eighteen patients only (Figure 2). The tumor size was 6 cm and 5 cm in the patients on pre-operative CT. Operation notes and pathological reports confirmed these findings (Figure 3). The two patients with a pre-operative diagnosis of tumor and stone underwent a radical nephrectomy whereas sixteen patients underwent simple nephrectomy. In the sixteen patients who underwent simple nephrectomy, one had duodenal injury and two sustained colonic injury. All of them were repaired and patients had uneventful postoperative recovery. Six of the sixteen patients underwent relook surgery after obtaining the histopathological diagnosis. In all the cases, the disease had become inoperable due to large nodal deposits (4/6) and fixed local mass (2/6) (Figure 4). Three patients underwent Postoperative Radiotherapy. Five patients received adjuvant Chemotherapy. Two patients with TCC received MVAC (Methotrexate, Vinblastine, Adriamycin, and Cisplatinum) therapy, while three patients with SCC received combination chemotherapy with Cisplatinum, Bleomycin and Etoposide. In the pathological details, the patient with adenocarcinoma had well differentiated tumor with no lymphovascular invasion and no nodal involvement. In the two patients with TCC, one had a high-grade tumor with nodal involvement. The second patient had low-grade tumor and nodal involvement was absent. In the SCC group, 9/15 patients had well differentiated tumor with keratin pearl formation (Figure 5), 6/15 patients had poorly differentiated tumors. All the patients had locally advanced tumor (T4). None of the eighteen patients developed systemic metastases. There were no areas of sarcomatoid differentiation in any of the tumors. The survival analyses were calculated for the different tumors and are given in a tabular form (Table 1). Discussion Primary neoplasms of the renal pelvis are uncommon and most are malignant. The majority of these cases consist of Transitional cell carcinoma (TCC). Pure SCC is very uncommon, though it is the second most common tumor in the renal pelvis.3 Only 350 cases have been described in literature.4 SCC is often associated with renal calculi or infection and it usually presents at an advanced stage with pain or palpable mass.5 The incidence of coexisting urinary stone disease varies from 18% in the United States to 100% in Hong Kong.5,6 In our series the association of SCC with calculus was 100%, which matches the data from the other Asian Series.5 We presume that this discrepancy may be due to difference in environmental conditions, and this needs further investigations. In the clinical features, we found that pain was the predominant feature in our patients. Six patients presented with haematuria. Of these six, two had gross haematuria and had tumor diagnosed on preoperative imaging study. In four patients, the haematuria was minimal, and preoperative ultrasound could not pick up tumor. So we think that the presence of haematuria in these patients should raise the suspicion of renal tumor. Another clinical feature that merits discussion is the presence of fever. Lytvunets in a retrospective analysis inferred that patients with keratinising squamous cell carcinoma were fever free.7 This may be an exception, since in our series; almost all patients had fever. This could be attributed to the presence of chronic renal infection from stone disease. There were no paraneoplastic syndromes in our series, which may be due to the advanced stage of tumors. Ultrasonographic aspects of renal pelvic tumors associated with stone disease have been described.8 The authors recognized echoic pelvic mass that was highly suggestive of urothelial tumor, though the correct preoperative diagnosis was rarely done. In the present series in only two patients we could see an echoic pelvic mass, which was highly suspicious of malignancy and this lead to the performance of a contrast enhanced CT scan. CT scan confirmed the presence of growth in both the cases. The primary outcome measure we wanted to test at the start of the study was the usefulness of CT scan in this patient group. As an accurate preoperative diagnosis is very important in this group of patients, this study conclusively proves the usefulness of CT imaging in long standing stone disease patients. The value of CT scan is unquestionable; the only controversy is regarding the timing and need for it. We cannot subject all stone patients to a screening CT. Such an endeavor will be fruitless and costly. In the present series we find that the average duration of stone disease is 8.8 years (6-11.6). An interesting aspect is that the moiety was non functional on a urogram and majority of them had haematuria. So we feel that a patient with long standing stone disease and associated poorly functional kidney or haematuria necessitates a screening CT. Table 1 depicts the survival data. It is obvious that patients who undergo complete radical extirpation of growth have survival advantage over patients who underwent incomplete resection. This grave prognosis in these patients urged us to study the biological behavior, hoping that earlier diagnosis and better outcome can be achieved in future. We feel that a screening CT done as per our recommendations would be cost effective, high yielding and beneficial test. This secondary outcome measure is the major strength of this study. By defining the need for a screening CT and the timing for such imaging, this study adds valuable evidence to the literature. Exhaustive literature search revealed no recommendation regarding the need and time for imaging studies in these patients. A screening CT would go a long way in improving the prognosis in this group of patients, thus having a positive effect in patient care. Further large multicentric prospective clinical trials in long standing calculus disease patients are needed in this direction to support out findings. We also tried to see if any pathological factor was responsible for the bad prognosis. Besides tumor stage we could not identify any other significant prognostic variable. The two major drawbacks of the study can be presumed to be the small numbers and the inclusion of three histological types of tumors. Although more than 350 cases of SCC of renal pelvis have been reported, there is only one study in literature which has more than 20 cases from a single institute.4 The limited number of patients seen by individual institutes limits the ability to define better the characteristic features of this uncommon neoplasm. Though the association of SCC and AC with stones is well known, it may be felt that the inclusion of TCC is probably unwarranted. It may be possible that the association of TCC with stone is purely anecdotal. Detailed literature search revealed two interesting studies that prompted us to include TCC also. Kaufmann's landmark series of cancer in spinal cord injury patients on long standing catheters and where stones were significant risk factors included 6 cases of SCC and five with transitional cell elements. The second study by Bickel reported 6 TCC'S and 2 SCC'S in a similar group of patients.9,10 We have an interesting hypothesis to support the occurrence of TCC in these patients. As everyone agrees, an initiating event drives the epithelia in these patients to hyperplasia. Subsequently this hyperplasia can evolve into frank carcinoma (TCC) or it can become dysplastic due to further irritation and dedifferentiate into SCC and AC. Further large clinical trials are needed to validate our hypothesis. At present, we can't definitely say there is a strong association between stone and TCC, but we included these tumors thinking that future studies may bring out an associationship if any. To summarize, this study has shown that malignancies associated with stone disease have insidious onset of clinical symptoms and there is a fair incidence of squamous malignancies. The possible way to improve prognosis is early diagnosis by screening patients of long standing urolithiasis with a CT scan in order to pick up the associated malignancies. References
Copyright 2003 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn03017f5.jpg] [cn03017f4.jpg] [cn03017f3.jpg] [cn03017t1.jpg] [cn03017f1.jpg] [cn03017f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}