 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 40, No. 3, (July - September 2003) , pp. 120-122 Case Report Solitary Calvarial Metastases: An Unusual Presentation of Thoracic Neuroblastoma Grover SB, Pati NK,* Saluja S,** Bhowmik KT*** Departments of Radiodiagnosis, *Pediatric Medicine, **Haematology, ***Radiotherapy,
Vardhman Mahavir Medical College and Safdarjang Hospital, New Delhi - 110029,
India.
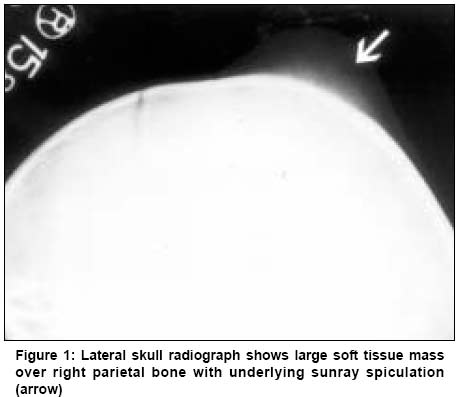
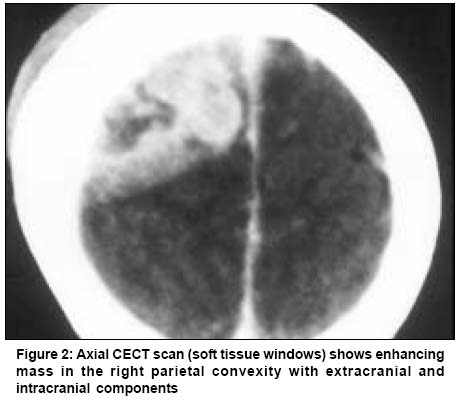
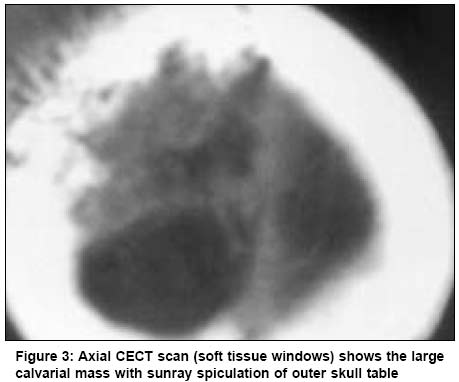
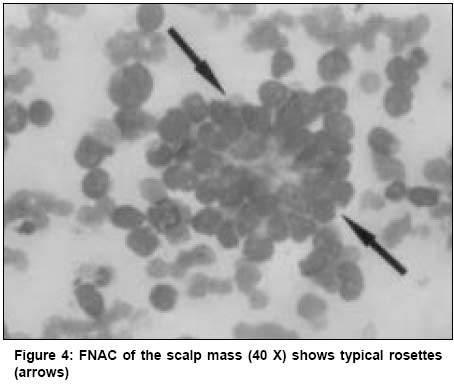
Code Number: cn03021 ABSTRACT: A primary thoracic origin occurs only in 20% of neuroblastomas, and their classical presentation is mediastinal or cord compression. Skeletal metastases of neuroblastomas are characteristically multiple, and calvarial deposits usually show simultaneous involvement of orbit. Solitary metastases in neuroblastoma, is an unusual entity and its presentation as a large calvarial mass, especially from a thoracic primary, is rare. Furthermore, calvarial metastases are relatively uncommon in children compared to adults. We discuss the clinical, radiographic, CT features, and differential diagnosis of a large calvarial mass with sunray spiculation in a child, which was due to a solitary metastases from an occult thoracic neuroblastoma. The possibility of neuroblastoma presenting in this unique fashion and the importance of considering a chemosensitive tumor such as neuroblastoma in the differential diagnosis of a solitary calvarial mass in a child is highlighted by our report. Key Words: Thoracic neuroblastoma, Metastases, Calvarium, Radiography, CT, Sunray spiculation. Introduction Neuroblastoma constitutes 10% of all pediatric malignancies and 75% of them present in children below 4 years of age.1 75% of neuroblastomas arise in the abdomen and pelvis, 20% in the thorax and 5% in the neck.2 Metastases in neuroblastoma characteristically occurs in a disseminated fashion the common sites being liver, lymph nodes, bones and bone marrow.1 The presentation of thoracic neuroblastoma with skeletal metastases is uncommon, due to its earlier presentation with mediastinal or cord compression, but is often observed in abdominal and pelvic neuroblastomas.2 Skull vault metastases are generally more common in adults and infrequent in children. Calvarial metastases however, do occur in neuroblastoma and are characteristically multiple lesions with simultaneous involvement of the orbits.3 The leading presentation of a neuroblastoma, as an isolated large calvarial metastases with sunray spiculation, is rare and has been described only once earlier by Egelhoff and Zalles in 1996, with the primary tumor originating in the adrenals.1 We report the clinical and imaging features of a similar case of an isolated calvarial metastases, however, in our patient the primary was in the thoracic paraspinal region. Case Report A 5-year-old male child presented with a history of gradually increasing scalp swelling over the right parietal region for 3 to 4 weeks and headache for 2 weeks. There was no history of trauma, convulsions, vomiting, limb weakness, abnormal bleeding or bladder / bowel disturbances. On examination the child was pale, had an average build, there was no lymphadenopathy or organomegaly. Local examination revealed a hard swelling of size 7 x 8 x 8 cm over the right parietal region, with fixity to the underlying bone. There was no tenderness or signs of inflammation over the swelling. Neurological examination revealed paraparesis with a muscle power of grade (IV/VI) in both the lower limbs. There was no sensory disturbance and no sensory level was recorded. A clinical diagnosis of a malignant skull and spine disease was considered and radiographs of the skull and spine were requisitioned. Skull radiographs revealed a 5 cm region of sunray spiculation in the right parietal bone, underlying the scalp swelling (Figure 1). Radiographs of the spine revealed a well defined para vertebral shadow at Dorsal 4 to Dorsal 5 level with a collapse of Dorsal 4 vertebra. Sonographic evaluation of the abdomen was normal. Laboratory investigations revealed : hemoglobin-6.8gm%, TLC-8.9 x 103/µl, DLC _ P52 L38 E6 M3 B1, and a normal peripheral blood picture. Contrast CT of the head revealed an enhancing extracranial tumor in the right parietal region, extending intracranially. The intracranial component had lobulated margins convex to the brain surface. There was no edema or midline shift in adjoining brain (Figure 2). Bone and soft tissue windows showed "sunray spiculation" of skull vault under the extracranial mass. (Figure 3). CT of dorsal spine confirmed para vertebral mass at D4 with vertebral destruction. Contrast CT of the abdomen was normal. A fine needle aspiration biopsy (FNAB) from the scalp swelling and a CT guided biopsy from the para vertebral lesion were obtained and the observations of both biopsies were similar. Cytological studies with Giemsa stain, revealed highly cellular smears with predominant small round cells, which had a monomorphic appearance with minimal nuclear pleomorphism. Individual cells were moderate in size with scant non-vacuolated cytoplasm. Characteristic rosettes with a central pink fibrillary material were recognized. There was no necrosis, calcification, ganglion cells or rhabdomyoblast (Figure 4). The appearances were diagnostic of neuroblastoma. Urinary VMA levels and bone marrow examination were normal. Radiographic skeletal survey and Tc 99 MDP bone scan did not reveal any additional tumors. A diagnosis of a primary thoracic paraspinal neuroblastoma with a solitary metastases in the skull vault was made. The patient was managed with a combination of chemotherapy and radiotherapy. Radiotherapy was given by Cobalt 60, 80cm SSD to a dose of 20 Gy in 8 fractions to the skull and the spine. Chemotherapy was given 3 weeks after completion of radiotherapy using a modified OPEC regime (Injection vincristine 1.5 mg/m2 intravenously, given on day 1, injection cyclophosphamide 600 mg / m2 intravenously, given on day 1, injection cisplatin 100mg/m2 intravenous infusion given after adequate hydration on day 2, and injection etoposide 1000mg/ m2 intravenously on day 4, with cycles being repeated every 21 days). Complete hemogram including platelet count was done prior to each cycle. The patient received 4 cycles of chemotherapy and no grade 4 toxicity was observed. The scalp swelling reduced in size and the paraparesis improved. Ultrasound and CT scan following the radiotherapy and chemotherapy did not reveal any additional tumors. The patient was lost to follow up after 5 months of treatment. Discussion The most common clinical presentation of a neuroblastoma is an abdominal mass. The characteristic presentation of a thoracic neuroblastoma however, is with tracheal / mediastinal / or cord compression. Metastases may also be the primary presentation of neuroblastoma and the common sites of such manifestations are liver, lymph nodes, bone and bone marrow.1 The skeletal sites of predilection for metastases are skull, facial bones, pelvis and proximal long bones.2,4 The characteristic radiographic pattern of skeletal metastases in neuroblastoma is of permeative destruction.4,5 Calvarial involvement in neuroblastoma is also classically of multiple lucencies, other patterns being diastasis of cranial sutures and "sunray spiculation" or a "hair brush appearance".1,5 The latter is a rare presentation, known to have poor prognosis with early death.1 An isolated calvarial deposit with a large soft tissue component and sunray spiculation as a leading presentataion of neuroblastoma has been described only once earlier by Egelhoff and Zalles.1 Spiculated new bone formation has also been reported in a mandibular metastases of neuroblastoma by Haddad et al.4 Our patient also presented with an isolated calvarial metastases which had spiculated bone reaction. The differential diagnosis in a child with a solitary calvarial mass and underlying osteolysis includes, osteomyelitis, eosinophilic granuloma, and malignant deposits from leukemia or lymphoma. Spiculated new bone formation is a feature usually characteristic of metastases from leukemia, lymphoma, melanotic prognoma, osteosarcoma or Ewing's sarcoma, rather than neuroblastoma.1 Since calvarial metastases are uncommon in children compared to adults, a primary pathology and surgical resection may usually be considered clinically for a child with an isolated calvarial mass. Therefore it is evident from our report and from the two other cases cited above, that in such a setting, instead of planning surgical resection, an imaging search for an occult abdominal or extra abdominal neuroblastoma should be undertaken even in a child above 4 years. Management decisions would be affected by this awareness, as neuroblastoma is primarily a chemosensitive tumor for which surgery is unwarranted. References
Copyright 2003 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn03021f3.jpg] [cn03021f4.jpg] [cn03021f2.jpg] [cn03021f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}