 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 40, No. 4, (October -December 2003) , pp. 127-134 Summated Chemotherapy Dose-intensity versus Loco-regional Response in Locally Advanced Breast Cancer: Its Possible Implications Datta NR, Rajkumar A, Basu R Department of Radiotherapy, Sanjay Gandhi Postgraduate Institute of Medical Sciences,
Lucknow, India.
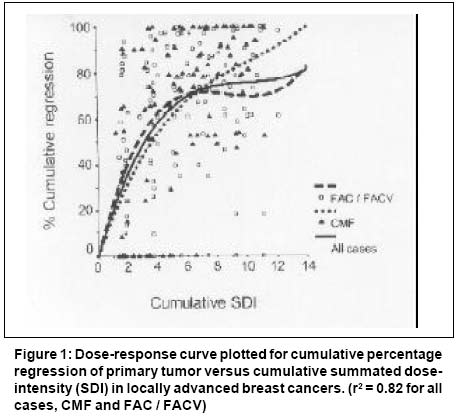
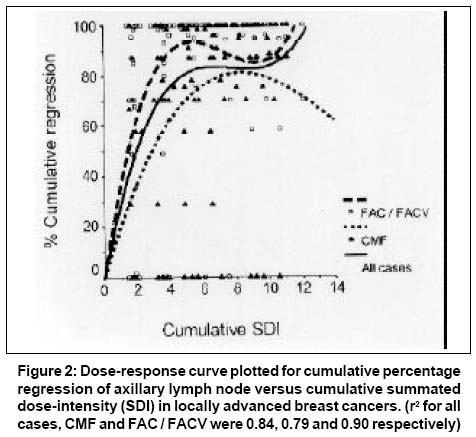
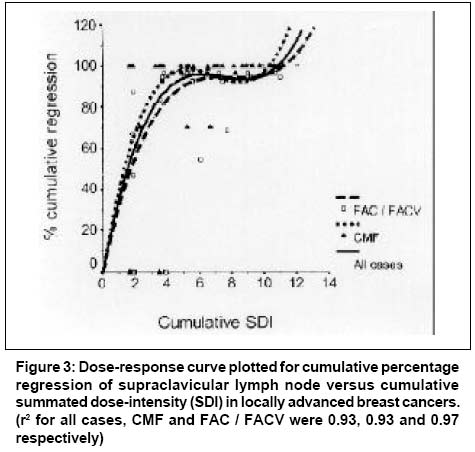
Code Number: cn03022 ABSTRACT: Background: Summated dose-intensity (SDI) of chemotherapy regimen could influence the outcome in malignancies. Aims: To evaluate the implication of SDI and identify key drugs for loco-regional response in locally advanced breast cancer (LABC). Settings and design: This retrospective study was based on audit of records of LABC patients who had received neoadjuvant chemotherapy (NACT). Material and Methods: Actual unit dose-intensity (UDI) of each drug and corresponding SDI of every doxorubicin (n=116 cycles) or non-doxorubicin (n=110 cycles) based NACT received by 42 patients of LABC were summated. Cumulative dose-intensity (CDI) for individual drugs and cumulative SDI (CSDI) for the entire course of NACT were estimated and correlated with quantum of primary tumor, axillary and supraclavicular nodal responses. Statistical analysis used: Two-sided chi-square, t-test, step-wise regression was used. Results: Dose-response curve between CSDI and corresponding responses for both primary and lymph nodes were sigmoid in shape for both doxorubicin or non-doxorubicin based NACT. Curves were best fitted using a cubic fit for all patients (r2 = 0.82, 0.84 and 0.93 for primary tumor, axillary and supraclavicular lymph nodes respectively). CSDI emerged as an important prognosticators for both primary (P<0.001) and nodal (P<0.001) responses. Individually, CDI of 5-fluorouracil for primary (P<0.001), CDIs of doxorubicin (P<0.001) and methotrexate (P=0.006) for axillary nodes and CDI of cyclophosphamide (P=0.001) for supraclavicular nodes were significant. Conclusions: Loco-regional responses in LABC are dependent on CSDI of NACT regimen. Drugs for high-dose intensification protocols could be identified and chosen based on the impact of CDI of individual drugs in NACT. Key Words: Dose-intensity, Dose-response, Locally advanced breast cancer, Neoadjuvant chemotherapy. Introduction Influence of dose-intensity of chemotherapy (CT) drugs and combination schedules has been regarded as one of the major determinants of outcome in breast cancer, both as adjuvant therapy and metastatic disease.1,2 The original concept of relative dose-intensity (RDI) proposed by Hryniuk and colleagues,3 was later modified by them with the introduction of summation dose-intensity (SDI).4 Based on various historic trials, Hryniuk et al. have demonstrated a linear relationship between outcome and the estimated SDI of CT regimens for both metastatic and adjuvant therapy in carcinoma breast.4 Total responses to neoadjuvant CT (NACT) for locally advanced breast cancer (LABC) have usually varied from 60_90% depending on the chemotherapeutic regimens used.5 There is usually a favor for doxorubicin based CT, even though this has not been substantiated on phase III trials for LABC.6,7 Bonadonna et al.8 have shown that the response rate may not be related to the drug(s) regimen but may be linked with dose-intensity of the chosen regimen.9 Most of the trials conducted to correlate the outcome and dose intensities of the drug(s) have used fixed intensity of the proposed CT regimens, rather than actual dose intensities received by the patients during the entire course of treatment. The present study evaluates the loco-regional response in LABC during the course of NACT with the corresponding actual NACT dose-intensity of each individual patient. The exact doses of CT agents used and their duration have been used to calculate the SDI of each cycle. The objective responses during CT have been correlated with the cumulative summated dose-intensity (CSDI) with the dose-response curves for both primary tumor and nodes to identify the drug(s) or combination, which could have a greater impact on the down staging of LABC. Material and Methods Patient population This is a retrospective study based on the audit of records of patients of LABC treated with NACT between 1994 to 2000. Pre-treatment evaluation consisted of histopathological confirmation, mammogram, routine hematological and biochemical profiles, radiograph of chest and radionuclide scans of liver and skeletal system. Assays for estrogen receptor (ER) and progesterone receptor (PR) could not be undertaken in majority of the cases since these were not routinely available in our Institute during that period. Most of patients had either received CMF with cyclophosphamide (C) (500mg/m2, days 1 and 8, IV), methotrexate (M) (40mg/m2, days 1 and 8, IV) and 5-fluorouracil (F) (600mg/m2, days 1 and 8), or FAC with 5-fluorouracil (F) (500mg/m2, days 1 and 8), doxorubicin (A) (50mg/m2, day 1) and cyclophosphamide (C) (500mg/m2, days 1 and 8, IV). In some patients, vincristine (V) (1.4 mg/m2, max. 2 mg on days 1 and 8) was also used with FAC combination leading to a FACV combination. All the cycles were administered at four weekly intervals to a maximum of 6 cycles before considering the patients for surgery. The choice of CT was based on individual physician preferences and patient's affordability (CMF being considerably cheaper than FAC or FACV). Only those who fulfilled the following criteria were included for further analysis. These included _ (a) a minimum of 3 cycles of either CMF, FAC or FACV, (b) detail recording of the CT, patient's body surface area at each cycle, actual dates of administration of each drug along with their respective doses and (c) details of dimensions in two axes of the primary and axillary lymph nodes before treatment and at the beginning of each cycle of NACT. Thus, 42 patients of LABC fulfilling the above criteria were evaluated for further analysis. Patients were staged as per TNM staging of the American Joint Committee on Cancer.10 Two patients with simultaneous bilateral breast lesions at presentation were staged separately. Thus, 44 primary tumors were evaluated from 42 patients, while axillary nodes were present in 37 of these 42 patients. Of these 42 patients, 26 were staged as M1 disease. These were either due to presence of supraclavicular nodes (n=13) or spread to other distant organs namely - liver, bone or lungs (n=12). One patient had disease spreading to the skin of the opposite breast. Twelve of these M1 patients received CMF while the remaining 14 were treated with FAC/ FACV regimens. Patients with bony secondaries also received palliative radiation to the involved site. Calculation of the tumor volume and response assessment The primary and the lymph nodes were measured clinically throughout the study using vernier calipers. Respective volumes were calculated from the two orthogonal diameters (in cm) _ "a" and "b" using the expression:11 Tumor volume (cu cm) = πab (a+b) / 12. Responses were quantified prior to the start of each cycle of NACT and expressed in terms of percentage change with respect to the pre-treatment volume. Tumor response was classified as complete response (CR) if there was complete disappearance of tumor; partial response (PR) for more than 50% regression; stable disease if the decrease was less than 50% to an increase of less than 25% in the size of the lesion; while any increase of greater than 25% of the diameter or appearance of new lesions were considered as disease progression. Calculation of cumulative summated dose-intensity Summated dose intensities were calculated as per the method proposed by Hryniuk et al.4 Thus the dose-intensity of each drug in each cycle was calculated as: Dose-intensity = Amount of the drug administered in each cycle / (body surface area x duration of the cycle in weeks x unit dose intensity of the drug). Unit dose intensity (UDI) values of the drugs in mg/m2/week were summarized by Hryniuk et al.4 as 650 for cyclophosphamide, 12.5 for doxorubicin, 700 for 5-fluorouracil, 20 for methotrexate and 2 for vincristine. In case of vincristine, 0.3 was deducted before dividing by the UDI. The individual drug intensity was estimated as per the actual doses received by each patient, with corresponding body surface and exact duration of the concerned cycle. These were summated to obtain the SDI of the combination protocol for each cycle. Since the effect of NACT on the total response at primary and nodes were a combined effect of the SDI dose intensities of each of the NACT cycles, individual SDIs of each cycle were summated to derive CSDI for the combination CT protocol for each patient. This was used to generate dose-response curves and run regression models for percentage response. Moreover, the cumulative dose-intensity (CDI) for individual drugs was calculated by summation of the dose intensities of each drug during the entire course of NACT. Thus, Cycle = n Cycle = n
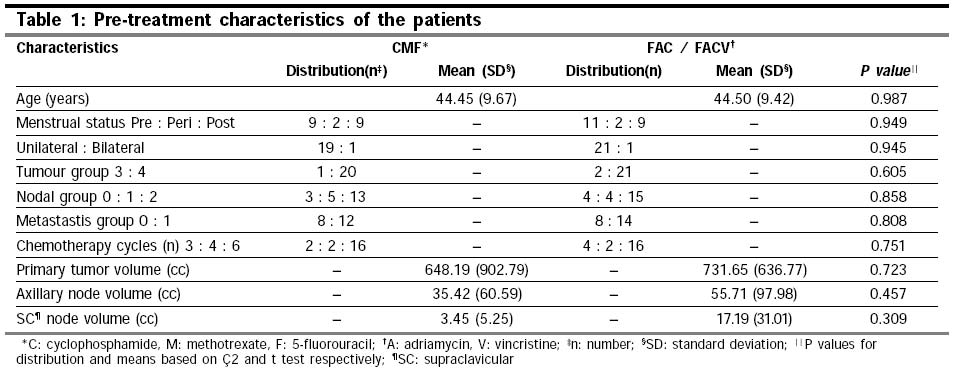
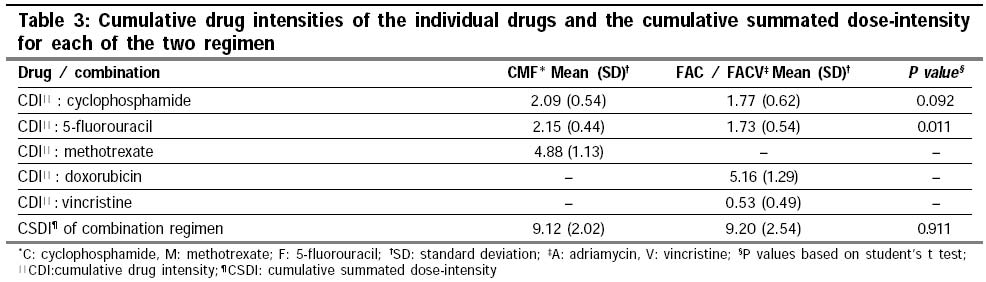
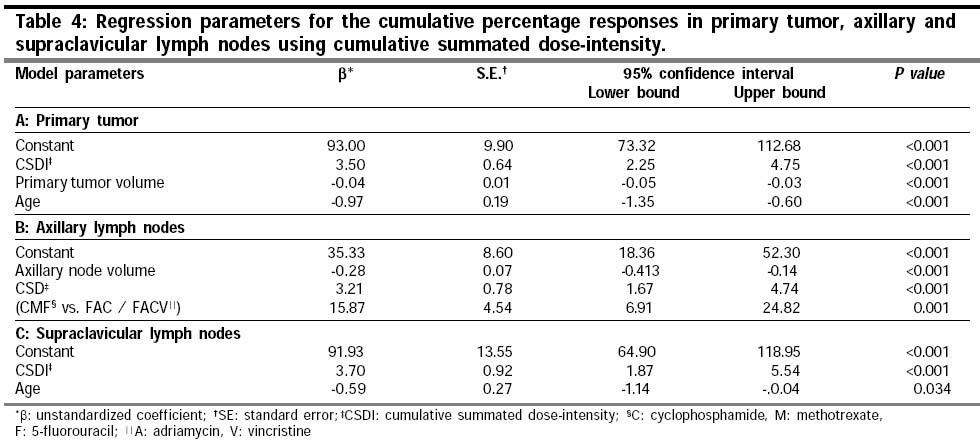
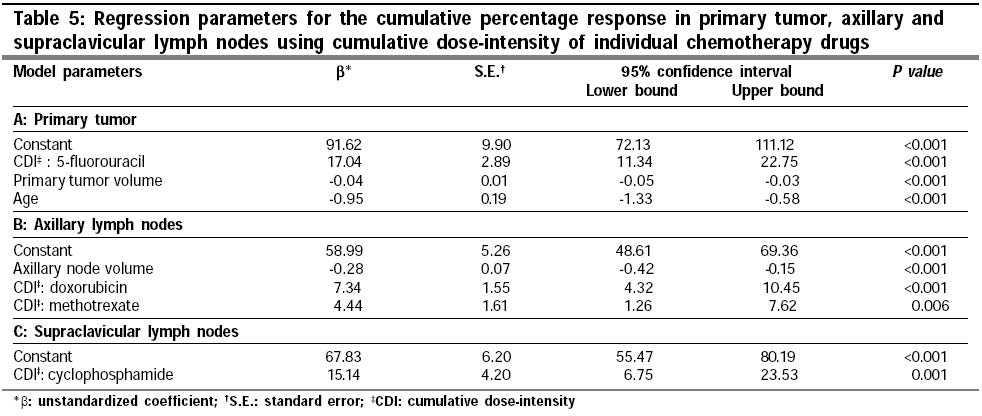
Statistical analysis Patients were grouped into either those treated with non-doxorubicin based CT (CMF) or doxorubicin based CT (FAC or FACV). Two-sided chi-square was used to test the significance of the frequency distribution of relevant parameters while the significance of means was tested by "two-tailed t test". Parameters influencing the cumulative response for primary tumor and lymph nodes were determined separately by linear regression using forward step wise regression with probability of F to enter being < 0.05 and removal at >1.0. The scatter plots were fitted using a cubic fit and regression coefficients, r2 were estimated for the total population and separately for the two groups of NACT. All statistical calculations were performed using SPSS version 9.0 (SPSS Inc. Chicago, IL, USA) for Windows. Results Patient demography Of the 44 primary tumors from 42 patients considered for response evaluation, 20 had received CMF while 22 were administered FAC / FACV. In doxorubicin based CT group, FAC was administered to 9 while 13 patients received FACV. One of the patients with bilateral tumors received CMF while the other received FACV. Patients on CMF and FAC / FACV had similar demographical profiles with respect to major patient related features. Out of 42 patients, all the seven patients in which ER and PR receptors were assayed; they were all reported as negative. All these patients had received FAC / FACV. Thus, hormone receptor assays could not be evaluated as a prognostic variable for tumor response to NACT between the two groups. Primary tumor and nodal volumes had shown a wide variation, but differences of their means were not significant between the two groups (Table 1). Loco-regional response to chemotherapy Loco-regional responses were quantified separately for primary and axillary lymph nodes. In 42 patients, for dose-response quantification, 110 cycles of non-doxorubicin NACT was administered in 20 patients, while 116 cycles of doxorubicin based NACT was administered in 22 patients. Although volumes for the primary tumor, axillary and supraclavicular lymph nodes were different, the corresponding mean volumes were not significantly different for patients treated with either CMF or FAC/ FACV regimes (Table 1) Of the 44 primary tumors, 85.7% (18/21) and 82.6% (19/23) of the primaries responded to CMF and FAC / FACV respectively (P=0.600). Four patients (19%) on CMF and 2 (8.7%) on doxorubicin based CT had a CR at primary site. Similarly, for axillary nodes, the total response (CR + PR) was 77.7% (CR=38.9%) with CMF and 94.7% (CR=52.6%) with doxorubicin based NACT (P=0.306). The mean total percentage regression at primary site by CMF and FAC / FACV was 71.4% and 66.1% respectively (P=0.624). For axillary nodes, it was 73.4% and 88.8% (P=0.146) with CMF and FAC / FACV respectively (Table 2). All the supraclavicular nodes responded to NACT irrespective of the regimen used. There was complete regression of nodes in 4 out of 6 patients (66.6%) with CMF and in 5 out of the 7 (71.4%) treated with FAC/ FACV (P=0.853). The mean total percentage regression was 99.1% and 98.7% with CMF and FAC / FACV respectively (P=0.681) (Table 2). Cumulative SDI and dose-response The dose-response curves between CSDI and corresponding responses at primary and the nodes were sigmoid and nearly similar for patients treated with CMF or FAC / FACV combinations (Figure 1, Figure 2 & Figure 3). The curves were best fitted using a cubic fit for both primary and nodes and exhibited an initial steep dose-response relation with CSDI before tending to plateau. The steep gradient in the dose-response was almost at half way of the CSDI delivered, corresponding generally to the dose received by 3 cycles of NACT. Although the drug combinations used in CMF and FAC / FACV were different, the mean CSDI ( + SD) received by the 2 groups were similar (P=0.911) (Table 3). The mean CDI for cyclophosphamide was marginally higher with CMF (P=0.092), while patients on FAC / FACV had a significantly higher mean CDI of 5-fluorouracil (P= 0.011). Factors influencing the loco-regional response to NACT On introducing CSDI along with other possible factors like age, menstrual status, T, N, M stages, tumor volume and the 2 groups of NACT-CSDI, primary tumor volume and age emerged as the most significant determinants for the primary tumor response. A higher CSDI, lower primary tumor volume and younger age appeared to favor primary tumor response to NACT irrespective of the type of CT combination used (Table 4). For axillary nodal response _ axillary node volume, CSDI and the type of CT combination emerged as primary prognosticators. Patients with smaller axillary nodes and higher CSDI had greater response to NACT. Moreover, doxorubicin based combinations had a significant edge over the CMF combinations (Table 4). For supraclavicular nodal responses, the CSDI of cyclophosphamide and age of patients were significant. Patients with younger age had a better supraclavicular nodal response (Table 4). Individual CDI of each drug was introduced into the regression model in place of SDI to identify drug/s principally influencing the responses in primary tumor and nodes. The drugs, which did not form part of combination CT (doxorubicin in CMF, methotrexate in FAC/FACV, vincristine in CMF and FAC) were not removed, from the regression model but considered as zero since the regression program would otherwise consider these drugs as missing leading to the removal of corresponding cases entirely from the regression model. Thus, for primary tumor response, CDI of 5-fluorouracil emerged as the key drug along with primary tumor volume and age. In case of axillary nodal response - axillary nodal volume and CDIs of doxorubicin and methotrexate appeared as the primary determinants while it was age and CDI of cyclophosphamide for supraclavicular nodal response (Table 5). Discussion Chemotherapy in breast cancer has been recognized to play an important role in all the three settings _ neoadjuvant in LABC, definitive for metastatic disease and as an adjuvant to surgery and radiotherapy. A number of drugs, both as single agent or as combinations and with diverse dosage schedules have been used in different settings. Comparisons to find out the best possible CT have perhaps been elusive due to the various permutations and combinations used in a wide variety of the patient groups.12,13 However, following various large-scale randomized trials, it is widely accepted that benefit of CT is certainly dose dependent and therefore should be administered in standard doses.1,14 Hryniuk and Bush3 introduced the concept of dose-intensity and had effectively shown the positive value of dose-intensity in relation to the treatment outcomes in stage II breast cancer, advanced breast and advanced ovarian cancers.15 More recently, using the concept of SDI, Hryniuk and co-workers4 compared different intensities of different CT regimes in breast cancer and demonstrated its utility on the basis of results from phase II and phase III trials reported in the literature for metastatic disease response and adjuvant trials. However, it would be of interest to explore the relative impact of SDI for NACT in LABC. Further, the correlation of SDI with outcome parameters as reported by Hryniuk et al.4 were based on CT protocols that were to be used in a given study. Since the entire concept of SDI revolves around the dose of chemotherapeutic agents actually administered in a specified time, the outcomes should be evaluated in terms of the actual dose intensities received by individual patients. Modifications in form of a reduction of CT dosage or increase in time interval between the administrations of drugs would change the SDI from the one proposed in a protocol leading to different SDIs being received. Thiscould have a bearing on the outcome. The dose-response pattern in LABC has not been earlier reported in the literature.16 It is believed that maximum shrinkage is usually observed during the first three cycles of CT. The initial steep dose-response gradient of the dose-response curves confirms this observation for both primary tumors, axillary and supraclavicular lymph nodes, irrespective of the combination used (Figure 1, Figure 2 & Figure 3). Since, SDI conceptually had brought all the chemotherapeutic agents on a single scale, similar SDIs should produce similar responses. This was evident from comparable responses at primary and lymph nodes due to the similar CSDI, irrespective of the NACT regime (Table 2 & Table 3). The impact of CSDI on the response rates was also evident as it emerged as the common factor to influence the loco-regional response. Doxorubicin based regimens had a selectively better impact on the axillary nodal response (Table 2 & Table 3). A wide range of drug combinations have been used for heterogeneous group of LABC, with different dose intensities which makes it difficult to pick up the ideal regimen.5,16 If one considers the UDI concept of different drugs, these drugs should then be producing similar responses if their UDI were similar. However, in this study, only cyclophosphamide and 5-fluorouracil were common to both protocols, of which CDI of the latter was significantly higher in the CMF patients (Table 3). Primary response was found to be significantly dependent on 5-fluorouracil, which explains the similar responses to primary site in this study, irrespective of the NACT regimen. Interestingly enough for axillary nodes, CDI of both doxorubicin and methotrexate appeared to influence the nodal response (Table 5). This could explain the non-significant difference in nodal responses between the two groups. For supraclavicular nodal regression, CDI of cyclophosphamide was the only agent of prognostic value. Cyclophosphamide or vincristine CDIs did not demonstrate any significantly direct impact on primary or axillary response. The NSABP B-22 trial also failed to demonstrate any influence of higher intensified doses of cyclophosphamide when used with doxorubicin in primary operable breast cancer,17 thereby concluding that dose-intensification of cyclophosphamide in doxorubicin-cyclophosphamide combination was not warranted for primary breast cancer. Similar conclusions were derived from the NSABP B-25 trial except for a subset consisting of women less than 50 years having 4 to 9 positive nodes.18 Dose intensification in carcinoma breast has been a subject of considerable clinical research.2,19 In a recent review by Piccart et al,2 the various drugs used for these intensification have been discussed and she concluded that perhaps increased doses of doxorubicin could be beneficial in biologically aggressive tumors especially those who over express c-erb B-2. However, it would be necessary to identify the drug/s that could be considered for dose intensification approaches. Recent results of the phase III multicentric trial comparing cyclophosphamide, epirubicin and 5-fluorouracil (CEF regimen) with a dose-intensified epirubicin, cyclophosphamide and filgrastim as NACT in LABC failed to demonstrate any benefit over the CEF.20 Similar findings have also been reported in another phase III randomized study comparing accelerated versus standard CEF versus CMF regimens in LABC.21 These negative results highlight the need of identifying the appropriate drug/s could be used in dose intensification protocols for LABC. In developing countries like India, late presentation of the disease coupled with financial constraints and patient compliance, effective management of LABC is a challenging task.22 There have been reports of use of alternate regimens like mitoxantrone, mitomycin C and methotrexate (MMM regimen) in LABC with reasonable success which are comparable to doxorubicin based NACT.23 The present study has attempted to identify such agents, which could be used for dose intensification protocols for NACT in LABC. It appears that 5-fluorouracil, one of the least expensive chemotherapy agents could be explored in such protocols for LABC, especially for primary tumor down staging. The study validates the SDI concept proposed by Hryniuk and co-workers4 for LABC and attempts to evaluate the aspects of dose intensification more critically based on the actual drug received, rather than just the SDI of protocol design. However, in view of the retrospective nature of this study involving small patient population, it would be appropriate to formulate prospective studies with a larger sample size to be able to identify drugs that could be considered for NACT dose-intensive protocols for LABC in the near future. References
Copyright 2003 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn03022f3.jpg] [cn03022t4.jpg] [cn03022t1.jpg] [cn03022t3.jpg] [cn03022t5.jpg] [cn03022f2.jpg] [cn03022t2.jpg] [cn03022f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}