 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 41, No. 1, (January-March 2004) , pp. 3-7 Neoadjuvant Chemotherapy in Squamous Cell Carcinoma of the Esophagus using Low Dose Continuous Infusion 5-Fluorouracil and Cisplatin: Results of a Prospective Study Aroori S, Parshad R,* Kapoor A,** Gupta SD,*** Kumar A,* Chattophadyay TK* Cancer Research Centre, Queen's University Belfast, U-Floor, City Hospital,
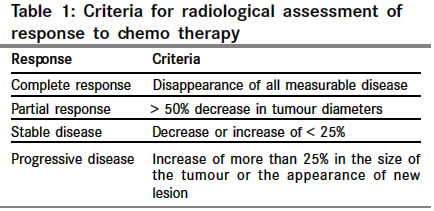
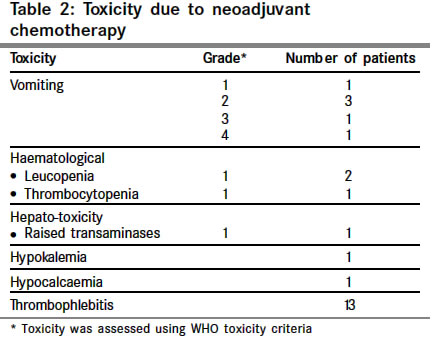
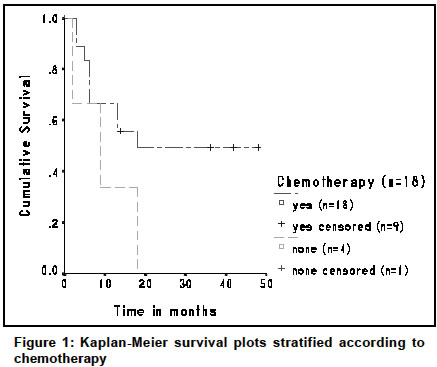
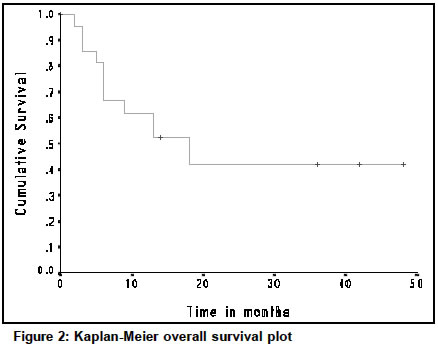
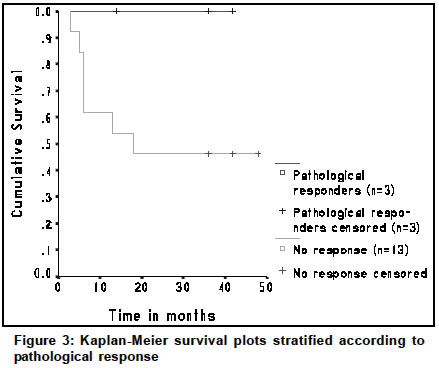
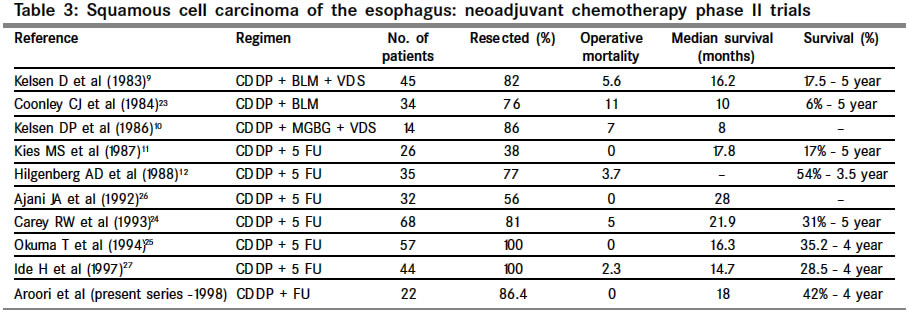
Belfast BT9 7AB; Code Number: cn04001 ABSTRACT BACKGROUND: Surgery is the treatment of choice for localized esophageal squamous cell carcinoma (ESCC). Despite curative surgical resection, the majority of patients develop local and systemic recurrence with poor 5-year survival. AIMS: To study the role of low dose continuous infusion (CI) 5-fluorouracil (5-FU) and cisplatin as neoadjuvant chemotherapy in ESCC. SETTINGS AND DESIGN: A non-randomized prospective study conducted over a period of two years (1996-1998) in the Department of Surgery, All India Institute of Medical Sciences, India. MATERIAL AND METHODS: Twenty-two patients with ESCC were included in the study. Chemotherapy consisted of a continuous 30-day infusion of 5-FU (350 mg/m2 /day) and cisplatin (7.5 mg/m2/day), 5 days/week for 4 weeks. All patients had surgery following chemotherapy. RESULTS: A full course of chemotherapy was completed in 18 patients (82%). Chemotherapy was not completed due to non-compliance (n=2), thrombophlebitis (n=1), and vomiting (n=1). Grade-1 haematological and hepato-toxicity was observed in four patients. Thirteen patients developed thrombophlebitis. After chemotherapy, improvement in dysphagia was observed in 13 of 22 (59%) patients. Radiological partial response was observed in 8 patients (36.4%). 19 patients underwent surgical resection (86.4%) with zero mortality. Post-operative morbidity was observed in six patients (27%). Complete and partial pathological response was observed in two (11%) and one patient (5.5%) respectively. The overall median survival was 18 months and 4-year survival was 42%. CONCLUSIONS: Low dose CI 5-FU and cisplatin is well tolerated with minimal toxicity. Histopathological response rates and survival figures are comparable with the more toxic neoadjuvant chemotherapeutic regimens. Key Words: Neoplasm, Esophageal cancer, Neoadjuvant Therapy, Fluorouracil, Cisplatin. INTRODUCTION Esophageal cancer is one of the ten most common malignancies worldwide.1 Squamous cell carcinoma of the esophagus (ESCC) is a common problem in several Eastern and Asian countries including some parts of India.2 Surgery is the treatment of choice for most localized esophageal cancer patients.3,4 Despite improvements in surgical techniques and reduction in post-operative mortality the overall outcome in esophageal cancer is poor with only 10% of patients surviving five years post-diagnosis.5 Between 40-60% of patients exhibit localized disease at diagnosis;6 however, the majority of those undergoing potentially curative resection will eventually succumb to metastatic disease.7-8 Pre-operative chemotherapy/chemo-radiotherapy has been used in an attempt to decrease tumour activity, increase resectability, and improve disease free and overall survival. There are reports which suggest improved resectability and survival using pre-operative chemotherapy.9-12 Randomized controlled trials comparing pre-operative chemotherapy with surgery alone13-16 showed a significant response in approximately 50% of patients, and significant down staging in the chemotherapy group. However, survival benefit was observed only in patients who responded to chemotherapy and toxicity appears to be a major problem in some of these studies.10,11,13,16 To minimize the toxicity associated with high dose bolus 5-fluorouracil (5-FU) and cisplatin and to evaluate the effect of combination chemotherapy we studied the role of low dose continuous infusion (CI) of 5-FU and cisplatin. MATERIAL AND METHODS The study was conducted between June 1996 and September 1998. Patients inclusion criteria were: 1) Age < 65 years, 2) Eastern Co-operative Oncology group performance status < 3, 3) measurable or evaluable disease, 4) squamous cell carcinoma of the middle or lower third or gastro-esophageal junction, 5) absence of metastasis, 6) no major concomitant infective, cardiovascular, neuorologic or respiratory diseases, 7) adequate haematological, hepatic, renal and pulmonary functions, and 8) informed written consent. Twenty-two patients with histological confirmed ESCC were enrolled into the study. There were 15 male and 7 female patients with a mean age of 48.3 years (range: 31-65). Tumour was located in middle third in 10; lower third in 11 and middle third with extension into lower third in one patient. Pre-treatment evaluation included full history and examination, full blood picture, hepatic, renal, and pulmonary function, 12-lead electrocardiogram, chest x-ray, oesophago gastroduodenoscopy (OGD), barium swallow and contrast enhanced computed tomography (CECT) of the chest and abdomen. All patients except those who did not receive a full course of chemotherapy had repeat OGD, barium swallow and CECT chest and abdomen following completion of chemotherapy. Full blood picture, liver and renal function tests were repeated twice a week until chemotherapy was completed. The chemotherapy schedule consisted of CI of 5-FU (350 mg/m2/day) over 24 hours for 30 days and cisplatin (7.5 mg/m2/day) in 200 ml of normal saline over 3 hours, 5 days/week for 4 weeks through a peripherally placed central venous line. Each patient was closely monitored for toxicity using the WHO criteria. Chemotherapy was stopped in patients who developed major toxicity, progression of the disease and in those who were non-complaint. All patients were operated within one to two weeks following completion of chemotherapy. Radiological response was assessed using Response Evaluation Criteria in Solid Tumours (RECIST) in those patients with measurable disease at base line. Measurable disease was defined as tumour masses that can be evaluated by computed tomography in which two perpendicular dimensions can be obtained and followed serially. The responses were classified according to the criteria in Table 1. Histological responses were divided into complete (no residual disease), partial (microscopic residual disease) or none (macroscopic residual disease). STATISTICAL ANALYSIS The overall duration of response was calculated from the start of treatment to disease progression and the survival times were calculated from the end of the treatment to death or last follow up, and censored at the last contact date in surviving patients. Survival curves were calculated by the Kaplan-Meier method using the Statistical Package for the Social Sciences (SPSS), version 11. RESULTS A full course of chemotherapy was completed in 18 (81.8%) out of 22 patients. A full course of chemotherapy could not be given for more than 15 days in four patients. Chemotherapy was stopped due to recurrent thrombophlebitis in one, grade-4 vomiting in one, and due to non-compliance in two patients. One of the non-compliant patients had complete relief of dysphagia by day 15 and refused further treatment. The most common toxicity was vomiting, grade-1 in one, grade-2 in three, grade-3 in one, and grade-4 in one patient. All patients, except one with grade-4 vomiting, responded to anti-emetic treatment. Haematological toxicity in the form of grade-1 leucopenia and grade-1 thrombocytopenia was observed in two and one patient respectively, which was resolved without any complication. Grade-1 hepato-toxicity (elevated transaminases) was observed in one patient and resolved without complication. Hypocalcaemia and hypokalemia was observed in one patient who responded to oral supplementation of potassium and calcium. (Details of toxicity are summarized in Table 2). In addition to vomiting the other major problem we encountered was the maintenance of the peripherally placed central venous line for 30 days. 13 patients (59%) developed thrombophlebitis and required change of the central venous line. Chemotherapy was stopped in one patient due to recurrent thrombophlebitis. Clinical improvement in dysphagia was noted in 13 (59%) out of 22 patients around the second week of chemotherapy. Dysphagia worsened in three patients, and chemotherapy was continued following feeding jejunostomy (n=2) and fluoroscopic guided nasogastric tube insertion (n=1). Endoscopic improvement was observed in 10 (45.5%) and post-chemotherapy CT showed a partial response in 8 (36.4%) out of 22 patients. All patients were offered surgery and the tumours were resected in 19 patients (86.4%). Twelve of the 18 patients who completed scheduled pre-operative chemotherapy had a Trans hiatal esophagectomy (THE) and four patients needed a Trans thoracic esophagectomy (TTE). Despite chemotherapy, tumours were unresectable in two patients and both underwent palliative substernal bypass. Three of four patients who could not complete chemotherapy underwent THE. The fourth patient, who refused chemotherapy after 15 days due to complete relief of dysphagia, was re-admitted to the hospital with progressive dysphagia at 6 months. The tumour was found to be inoperable at laparotomy. The average time for surgery was 3.30 hours; with average blood loss of 700ml. Thirty-day postoperative mortality rate was zero. Post-operative morbidity was observed in six patients (27%). Two patients in the resected group and one in the surgical bypass group developed anastomotic leak in the neck. Two patients in the TTE group had chest wound infection and one patient had chylothorax. The patients with neck anastomotic leaks were managed conservatively and all recovered uneventfully. The patient with chylothorax was operated on the same day of detection and recovered uneventfully. A complete pathological response (T0, N0) and a partial response (T0, N1) were noted in two (11.1%) and one patient (5.5%) out of 18 patients respectively. At the time of last follow up (December 2000), nine of 18 patients who completed scheduled pre-operative chemotherapy had died. Of the four patients who did not complete chemotherapy three had died at 2, 9 and 18 months respectively while one was lost to follow up (Figure 1). Analysis according to surgical procedure revealed that both patients who had substernal bypass died at 2 and 3 months respectively. Nine out of 16 patients who had curative resection are alive. Eight of them have a follow up of more than 3 years. Overall median survival was 18 months (Figure 2) and four-year survival was 42%. All three patients with complete/partial pathological response are alive with a follow up of 14, 36 and 42 months (Figure 3). DISCUSSION ESCC is associated with poor prognosis.5 Remarkable progress has been documented over recent decades with respect to the surgical treatment of ESCC.8,17 There is a need to improve long-term survival, particularly for those with locally advanced disease. Multi-modality therapy approach was introduced aimed at obtaining higher cure rates with less recurrence from occult metastases.18 There is a particular interest in neoadjuvant regimens because of initial results, which have suggested a potential benefit from this therapy.9-13,15,16 High-dose 5-FU in combinations with cisplatin are the most extensively used chemotherapeutic regimen in the treatment of carcinoma of esophagus. One of the major problem associated with this regimen is severe dose limiting myelosuppression, mucositis and nephrotoxicity.11,14,16 Several studies have suggested that continuous infusion of 5-FU is associated with minimal toxicity and improved response rates when compared to bolus 5-FU, in advanced head and neck,19 gastric,20 and colorectal cancers.21,22 The role of low dose CI of 5-FU and cisplatin in ESCC is not clear. Based on the encouraging results from above studies we decided to study the role of low dose CI of 5-FU in combination with cisplatin in patients with ESCC. Like in many previous studies we did not observe any grade-3 and grade-4 haematological toxicity in our series. Only three patients had grade-1 haematological toxicity and none required interruption of chemotherapy. Though vomiting was the most common side effect in our series (27%) treatment was interrupted in only one patient. Unlike in other series14 there were no drug related deaths in our series. Our surgical (resectability rate of 86.4% and zero mortality) results and histopathological response rates (11.1% complete response and 5.5% partial response) are comparable with results from many phase II neoadjuvant chemotherapy trials reported in the literature.9-12,23-27 Table 3 summarizes comparative results of various phase II studies of neoadjuvant chemotherapy for esophageal cancer. The median survival at the time of last follow up was 18 months and four-year survival was 42%. A four-year survival of 42% in our series compares favourably with that reported in the literature.9-12,23-27 To conclude, low dose CI of 5-FU and cisplatin was well tolerated with minor toxic effects. The response rates, resectability rates and survival figures compare favourably with that of more toxic conventional regimens published in the literature. One of the major drawbacks of our study is small sample size. However, the results of our study, in particular, minimal toxicity, absence of treatment related deaths, and 16% pathological response rate are significant when compared to other high dose 5-FU and cisplatin based regimens reported in the literature. Because of the small sample size and non-randomised nature of the study it is difficult to make any firm conclusions, but the observations, which were made here are important and low dose CI of 5-FU in combination with cisplatin in the treatment of ESCC needs further evaluation. REFERENCES
Copyright 2004 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn04001t1.jpg] [cn04001f3.jpg] [cn04001t3.jpg] [cn04001t2.jpg] [cn04001f1.jpg] [cn04001f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}