 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 41, No. 1, (January-March 2004) , pp. 13-17 Complete Axillary Conversion after Neoadjuvant Chemotherapy in locally Advanced Breast Cancer: A Step Towards Conserving Axilla? Arimappamagan A, Kadambari D, Srinivasan K, Krishnan R,* Elangovan S,** Reddy KSN*** Department of General Surgery, *Pathology, **Radio-diagnosis and ***Radiotherapy
JIPMER.
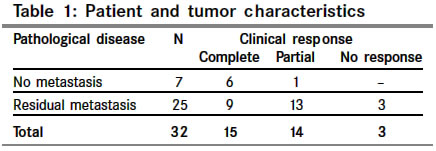
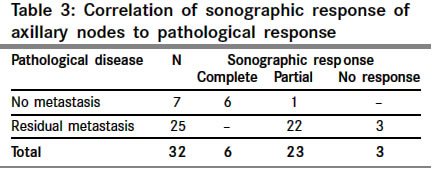
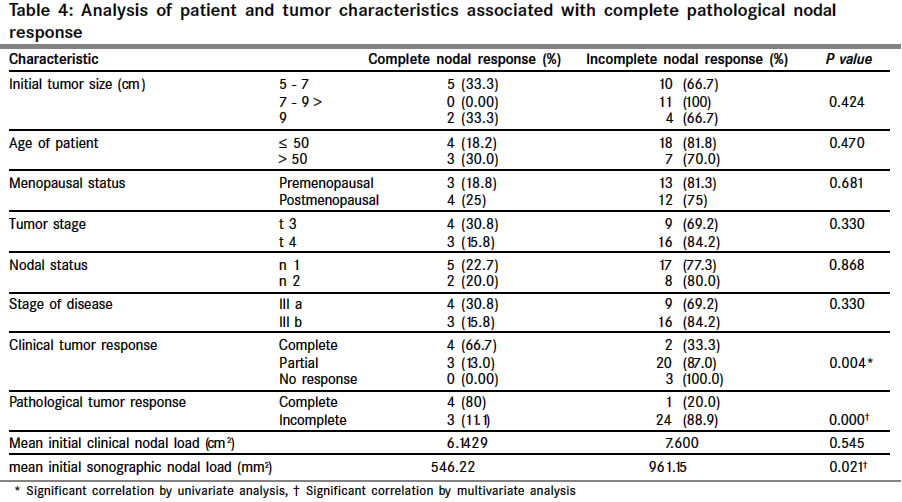
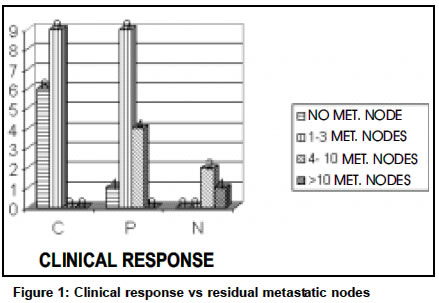
Code Number: cn04003 ABSTRACT OBJECTIVES: This study was designed to assess the clinical, sonographic and histopathological response of axillary lymph node metastasis to neoadjuvant chemotherapy in patients with locally advanced breast cancer. MATERIAL AND METHODS: Forty patients with locally advanced breast cancer (LABC) with clinically palpable or sonographically detectable axillary nodes were studied. FNAC of the primary tumor and axillary nodes was done and patients were started on neoadjuvant chemotherapy. Axillary nodes were assessed clinically and sonographically for response after 3 cycles of chemotherapy. All patients underwent total mastectomy with axillary clearance and the lymph nodes in the specimen were examined for metastasis. Results: 47% patients had complete clinical nodal response, while 19% showed complete sonographic response. Complete pathological nodal response was documented in 22% of patients. Ultrasonography was found to be more sensitive than clinical examination in assessing complete nodal response. 10% of the patients had complete pathological response of both primary tumor and axillary nodes. There was significant correlation between pathological response of primary tumor and lymph nodes (P=0.004). Patients with complete sonographic or clinical response were found to have no or minimal residual disease in axilla and hence axillary dissection may be avoided in them. Key Words: neoadjuvant chemotherapy, locally advanced breast cancer, axillary nodal response. INTRODUCTION The current trend in the management of breast cancer is towards breast conservation wherever possible. With the increasing use of neoadjuvant chemotherapy (NACT), this is becoming a distinct possibility for larger tumors as well. While neoadjuvant chemotherapy is the standard treatment for locally advanced breast cancer, recent studies and reviews attempt to address the issue of its use in early operable breast cancer.1 Axillary lymph node dissection is still the standard management for axillary nodal metastases. Sentinel lymph node biopsy after NACT is evolving as an alternative to axillary dissection.2 Many studies have assessed clinical response of axillary nodes to NACT. Some studies have demonstrated complete pathological response following neoadjuvant chemotherapy.3-5 Few studies however have addressed the issue of omission of axillary dissection in a subset of patients following NACT.1,3,6 This study was designed to assess the axillary nodal response to neoadjuvant chemotherapy by clinical examination, ultrasonography and by histological examination. The incidence of complete axillary conversion was documented. An attempt was made to correlate the tumor characteristics to axillary nodal response. MATERIAL AND METHODS The study included patients of LABC with clinically palpable or sonographically detectable axillary lymph nodes attending surgical OPD between August 2000 and May 2002. The work up included FNAC from primary tumor and axillary nodes, complete hemogram, biochemistry and electrocardiogram. Clinical staging of the tumor was done and the surface area of the primary tumor was calculated as the product of the two longest perpendicular diameters. The number and size of palpable axillary lymph nodes was noted. The sum of the products of two greatest perpendicular diameters of each node was obtained for the assessment as per WHO guidelines for reporting cancer research.3,7 Ultrasonographic examination of the axilla was done using GE.RT-3600 equipment with 7.5 Mega Hertz transducer probe. The number of lymph nodes in the axilla, their sonographic characteristics and their size in two longest perpendicular diameters were documented. The sum of their products, termed the sonographic nodal load, was calculated. Similar assessment was done after completion of chemotherapy. FNAC was done to establish the prescence of metastases in all patients. The node found clinically significant in terms of size and consistency was chosen in patients with palpable lymph nodes. In those with no clinical demonstrable nodes ultraound guided FNAC was done and well-defined hypoechoic nodes with an eccentric hilum or those producing distortion of the surrounding soft tissue were selected. All patients received three cycles of Adriamycin based chemotherapy at three weekly intervals. (CAFV on day 1 and 5FU on day 8; cyclophosphamide 500mg/m2, adriamycin 50 mg/m2, 5 flurouracil 500mg/m2, vincristine 1.5 mg/m2). All the patients were reassessed clinically for feasibility of surgery 21 days after the completion of the third cycle of chemotherapy. Ultrasonographic examination of the axilla was also done. Patients underwent total mastectomy with axillary dissection within one month after completion of the third cycle of chemotherapy. The pathological specimen was examined in detail for the number of lymph nodes and their metastatic status. Additional sections were taken in patients showing a complete pathological tumor or nodal response. The histological changes in individual lymph nodes were studied in detail. The clinical, sonographic and pathological response of the tumor and the axillary lymph nodes were documented and classified as per the WHO criteria7 namely, complete response (CR) meant disappearance of all known disease, partial response (PR) denoted decrease of 50% or more in total tumor load of lesions that have been measured to determine the efficacy of therapy and no response where 50% decrease in size could not be demonstrated. The pathological response was correlated to the clinical and sonographic assessment. The response of the tumor and the axilla were correlated with various patient characteristics and analyzed. The data was analyzed using SPSS 10.0 for WINDOWS software. Chi-square test and Fisher's exact test were used wherever indicated. The correlations were done by Spearman rank correlation analysis and the multivariate analysis done using regression model by analysis of variance (ANOVA). A `P' value of less than 0.05 was considered statistically significant. RESULTS Forty-seven patients with locally advanced breast cancer were inducted in the study. Forty patients completed the treatment protocol and were considered for the analysis. The patient and tumor characteristics are as shown in Table 1. The number of lymph nodes detected by clinical examination ranged from 0-5 (mean 2.17). The number of lymph nodes detected by ultrasonography ranged from 2-12 per patient (mean 5.95). Ultrasonography of axilla picked up significantly more number of nodes. The mean tumor load in axilla was greater by sonographic assessment than by clinical examination (7.795 cm2 and 6.57 cm2 respectively; P<0.001). Complete pathological response of primary tumor was noted in five patients (13%), four of who also had a complete clinical response. One had an ill-defined palpable residual mass. Menopausal status, initial stage of tumor or initial size of primary tumor did not correlate with the primary tumor response. Assessment of axillary nodal response Thirty two out of 40 patients, who had cytologically proven nodal metastasis before chemotherapy were included in the final analysis. Complete clinical nodal response was recorded in 15 patients (47%) and partial response in 14 (44%) (Table 2). On sonographic assessment of axilla, response was complete in 6 patients (19%), partial in 23 patients (72%) and no response in three patients (Table 3). The mean pre-chemotherapy sonographic nodal load significantly varied between patients with complete axillary conversion and those with residual metastasis (546.22 mm2 vs. 961.16mm2; P=0.029) (Table 4). Seven out of thirty two patients (22%) had no histological demonstrably disease in the axilla (Tables 2 and 3). Out of 15 patients with complete clinical response, six had complete pathological axillary conversion. The other nine (60%) with residual disease in axilla, however, had three or less metastatic nodes (Figure 1). All 6 patients with complete sonographic response had no residual disease in axilla (Table 3). One patient who had a clinically palpable node and sonographically detectable disease had no histological evidence of residual nodal disease. Menopausal status, initial tumor size or initial stage of the disease did not correlate with the pathological axillary nodal response (Table 4). Four patients had complete tumor and nodal response (10%) pathologically. One patient who had no histological residual disease in the breast had residual metastasis in axilla after chemotherapy. Residual disease in breast was noted in three patients who had complete pathological axillary conversion. We identified a group of patients (22%) with complete axillary conversion after neo-adjuvant chemotherapy. Univariate analysis demonstrated that complete pathological response of primary tumor, sonographic initial nodal load and clinical tumor response correlated significantly with complete pathological nodal response. Multivariate analysis demonstrated that only complete pathological primary tumor response and low prechemotherapy sonographic nodal load were predictive of complete axillary conversion (Table 4). DISCUSSION The present study confirmed that ultrasonography of axilla is better than clinical examination in the assessment of axillary nodes and their response to neoadjuvant chemotherapy. Herrada et al8 in their study comparing clinical examination, sonography and mammography concluded that sonography was the best single non-invasive method of assessing the extent of nodal involvement based on size of nodes. In our study, considering pathological assessment of the axilla as the gold standard, ultrasonography was found to be more sensitive than clinical examination for assessment of axillary nodal response (sensitivity 100% vs. 64%; specificity 86% vs. 86% respectively). The sensitivity and specificity of axillary ultrasound for assessing response in a study by Kuerer et al9 were found to be 62% and 70% respectively, when compared to physical examination, which had a sensitivity of 45% and specificity of 84%. They showed that the difference in sensitivity was statistically significant (P=0.012), whereas that of specificity not significant. The high sensitivity of axillary sonography in our study could be attributed to the definition of complete sonographic response as the absence of any detectable node in axilla. The study by Kuerer9 and Vlastos6 had considered the axilla to be positive only if it contained suspicious or frankly metastatic nodes, visualized as ovoid or lobulated, well demarcated, hypo echoic nodes (>5 mm). The axilla was considered to be negative for disease when it was reported to be without any visible adenopathy or to contain echogenic, fat replaced nodes.6 The sensitivity and specificity of ultrasonography for detection of axillary lymph nodes have been reported to range from 56% to 73% and 70 to 90% respectively.10-12 The absence of metastases in axillary nodes cannot be assumed based on the sonographic findings alone and therefore, we considered axilla to be positive with detection of any node sonographically. Our study documented complete axillary conversion in 22% (n=7) patients following neoadjuvant chemotherapy. Kuerer et al3 documented complete axillary conversion in 43 (23%) out of 191 patients who had cytologically documented nodal metastasis before receiving NACT. Previous studies have reported conversion of clinically involved axilla to a pathologically negative status in 25 to 38% of patients following neoadjuvant chemotherapy. The nodal metastasis was not cytologically documented before administering chemotherapy in these two studies.5,13 Documentation of metastasis in axillary nodes before initiation of chemotherapy, as done in our study, is essential to demonstrate complete pathological response following NACT. Clinically palpable nodes cannot be considered to be metastatic. In our study, we observed that eight patients who had clinically palpable nodes did not have metastasis. Axillary lymph node status has been known to be the single most important prognostic indicator in breast cancer,14-16 and is the chief indication for axillary dissection.15 However, axillary dissection is not without its attendant morbidity. It was noted that 82% of patients reported at least one upper limb complaint 3 months after surgery.17 Overall incidence of arm edema following axillary dissection was 20%.18 Morbidity from axillary dissection is more when compared to radiation alone.19 Hence, if axillary dissection can be avoided in some patients, it would prevent needless morbidity. Fisher et al found no survival difference in patients with microscopic disease who underwent either total mastectomy with regional irradiation or radical mastectomy.20 Various alternatives have been proposed for the treatment of axilla like axillary radiation6 and sentinel lymph node biopsy (SLNB).3,21 Vlastos et al found that most patients who are false negative by clinical or sonographic examination have only minimal residual disease and thus may be good candidates for axillary irradiation in place of axillary dissection.6 Most studies on the role of SLNB following NACT have documented that SLN could be accurately identified and could predict the status of the axillary lymph nodes in over 90% of patients.22,23 SLNB is advocated before use of NACT in clinically node negative patients as a means of reducing the false negativity rate. It allows for identification of node positive patients subsequently rendered disease free in lymph nodes, which can assist in planning additional radiation or chemotherapy. Sabel et al24 found residual nodal disease in 60% of patients who had positive SLNB prior to induction chemotherapy. We found that all patients with complete sonographic response (22%) had no residual metastases in the axilla. Previous studies reported that an axilla negative by clinical examination and sonography after induction chemotherapy still had 48 to 53% chance of being pathologically positive.6,9 This discordance in the sonographic assessment when compared to our study can be explained due to the difference in defining a negative axilla. In our study, patients with complete clinical nodal response were found to have residual metastases in 60% of them. All these patients were found to have three or less metastatic nodes (Figure 1). We suggest that axillary dissection can be avoided in patients with complete sonographic response. These patients would receive post-operative chemotherapy and axillary irradiation which can take care of any occult residual metastasis. Those with complete clinical nodal response had either no or minimal residual disease in the axilla. Whether this minimal residual disease can be treated with radiation and chemotherapy alone warrants further randomized studies. Sentinel node biopsy may be more useful in this group of patients. REFERENCES
Copyright 2004 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn04003t4.jpg] [cn04003t2.jpg] [cn04003t1.jpg] [cn04003t3.jpg] [cn04003f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}