 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 41, No. 1, (January-March 2004) , pp. 18-24 Tumor regression dynamics with external radiotherapy in cancer cervix and its implications Datta NR, Rajkumar A, Basu R Department of Radiotherapy, Sanjay Gandhi Postgraduate Institute
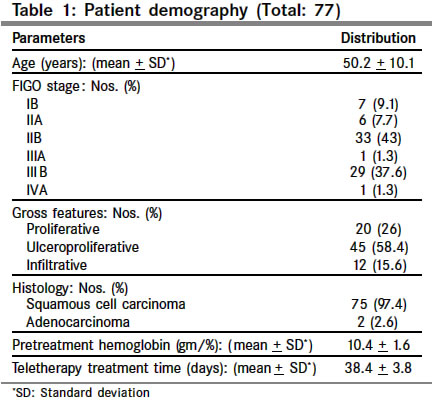
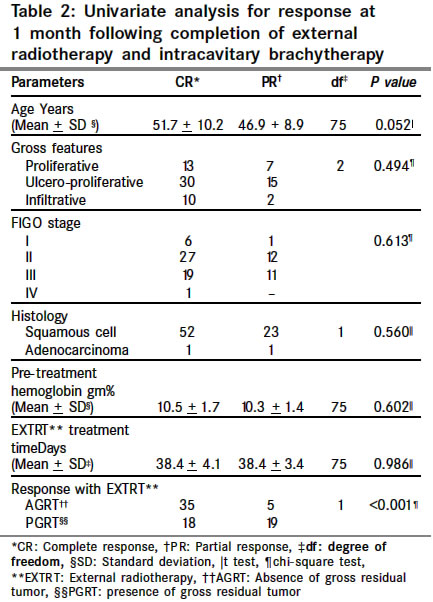
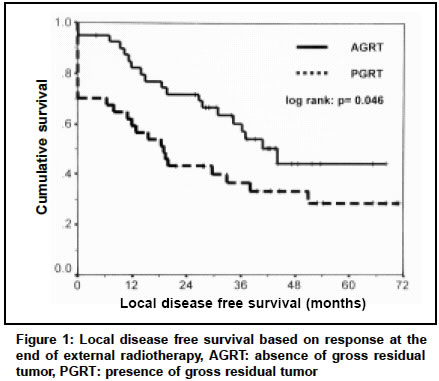
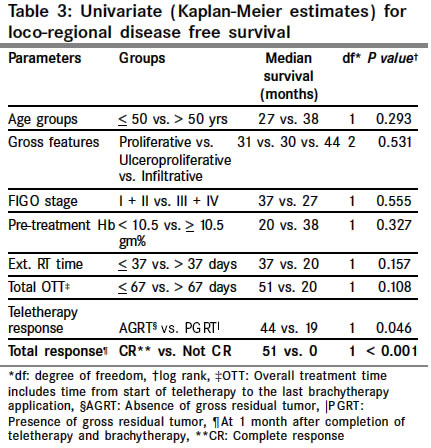
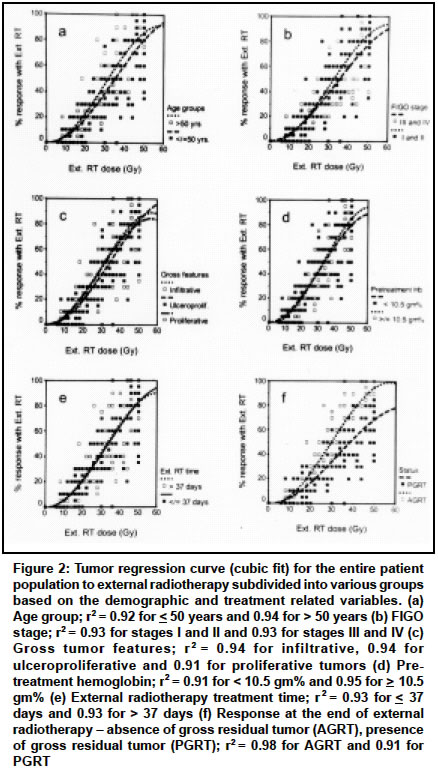
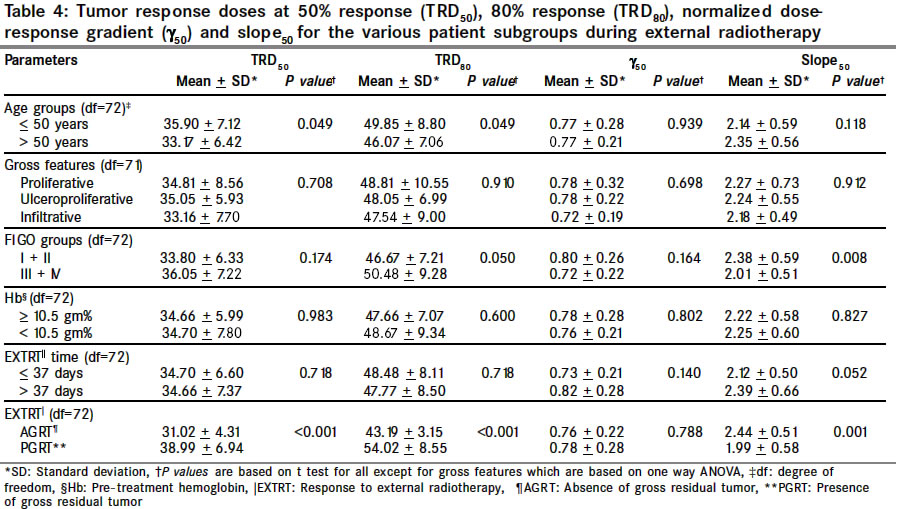
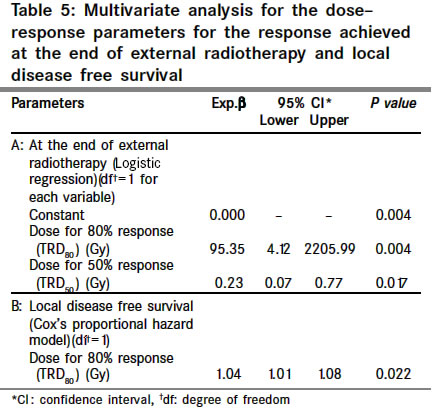
of Medical Sciences, Lucknow, India. Code Number: cn04004 ABSTRACT BACKGROUND: To study the external radiotherapy (EXTRT) regression patterns in cancer of the cervix. AIMS: Evaluate EXTRT tumor regression doses (TRD) for 50% (TRD50), 80% response (TRD80), normalized dose response gradient (g50) and slope (slope50) with clinical outcome. SETTINGS AND DESIGN: Patients, treated solely with radiotherapy and enrolled for other prospective studies having weekly tumor regressions recorded were considered. MATERIAL AND METHODS: Seventy-seven patients received 50Gy of EXTRT at 2 Gy/fraction followed by 18Gy of high-dose rate intracavitary brachytherapy at 6 Gy/fraction. Loco-regional regressions were assessed clinically at weekly intervals during EXTRT to generate EXTRT dose-response curves. STATISTICAL ANALYSIS USED: Student's t test, logistic regression, Kaplan Meier and Cox's proportional hazard model. Scatter plots were fitted using cubic fit. RESULTS: Age (P=0.052) and absence or presence of gross residual tumor (AGRT and PGRT respectively) following EXTRT (P<0.001) were the only determinants for complete response (CR) at 1 month following completion of radiotherapy. EXTRT tumor regression sigmoid curves obtained for various patient characteristics differed only for those with AGRT and PGRT with differences in TRD50, (P<0.001); TRD80 (P<0.001) and slope50 (P=0.001). Response status to EXTRT was a prognosticator for loco-regional disease free survival (LDFS) (AGRT vs. PGRT; P=0.046). On multivariate analysis, both TRD50 and TRD80 emerged as significant predictors for tumor status at end of EXTRT while TRD80 was the sole determinant of LDFS. CONCLUSION: Extent of tumor regression to EXTRT is an important predictor for treatment outcome in cancer cervix as evident from TRD50 and TRD80 values of EXTRT tumor regression curves. Key Words: Dose-response curve, Radiotherapy, Cervical cancer. INTRODUCTION External radiotherapy (EXTRT) forms an important component of management of cancer cervix. The dynamics of radiation induced tumor regression can be best evaluated using "S" shaped sigmoid dose-response curve.1-3 Although, there has been unanimity in accepting this relation to be sigmoid, difference of opinion exists about the best possible parameter to quantify this curve to carry an inter-comparison between the various studies.3-8 A major concern has revolved primarily around quantifying the position and slope of this sigmoid curve.4 The parameter widely accepted for defining the steepness is normalized dose gradient - g, proposed by Brahme.5 However, recently an alternative estimate of steepness has been proposed - slope50 and q50 (defined later).3,7 Bentzen and Tucker4 reviewed and highlighted the ambiguities that are associated with estimation of these parameters. A true sigmoid dose-response curve can be generated only if the various data points on clinical outcome are available for the entire range of the radiation dose, starting from a minimum to a maximum tolerable dose. It is ethically difficult to subject patients to such a wide range of doses in clinical situations, for constructing a dose-response relation over this entire range. Thus, majority of the data, which are available, are near maximum clinically acceptable doses for a given tumor.4,9 Perhaps one of the ways that could be explored to get a dose-response curve over a wide range of doses would be to look at the regression pattern of the gross tumor during a course of EXTRT. The present study has been carried out to establish the dose-response relation of primary tumor regression during the course of EXTRT in a group of patients of carcinoma of the cervix treated with an identical teletherapy and brachytherapy protocol. Outcomes were correlated with various demographic and dose-response parameters to identify the most relevant parameter of the sigmoid curve and recognize its implication in management of carcinoma of the cervix. MATERIALS AND METHODS Seventy-seven patients of carcinoma of the cervix were selected from the database of all patients of cervical cancer treated at our institution from January 1996 to June 2001. Before the start of therapy, all patients were subjected to routine clinical, hematological, biochemical and radiological investigations and staged clinically as per FIGO staging guidelines. The inclusion criteria were (a) patients who had received a planned EXTRT of 50 Gy at 2 Gy per fraction with 5 fractions per week followed by (b) high-dose-rate intracavitary brachytherapy (ICBT) of 18 Gy in 3 fractions at weekly intervals to Point A, started one to two weeks following the completion of EXTRT and (c) in those where periodic tumor responses at corresponding doses were available during the course of the radiotherapy. EXTRT was delivered by either telecobalt (Theratron 780C, AECL, Canada) or 6 MV / 10MV photons (ML 20DX, Mitsubishi Corporation, Japan). This was followed one to two weeks later by high dose rate ICBT (Microselectron HDR, Nucletron, The Netherlands or Ralstron 20B, Shimadzu Corporation, Japan). Loco-regional response at the primary and parametria were recorded as percentage regression from the pretreatment size. These were based on clinical evaluation namely, per speculum, per vaginum and rectovaginal examinations carried out during weekly monitoring of patients during the course of treatment. Even though, this forms a retrospective collection of cases, these patients had been part of other prospective studies, where weekly recording of tumor regression was mandatory. At the end of EXTRT, tumor responses were graded based on the criteria defined by Hong et al.10 and Chen et al.11 This includes (a) absence of any gross residual tumor (AGRT): complete or near complete regression of pelvic tumor, nonspecific, fibrosis, or granulation over cervix and (b) presence of gross residual tumor (PGRT): presence of gross residual tumor or palpable nodularity on cervix and / or palpable nodularity on the parametrium. At 1 month following completion of EXTRT and ICBT, all patients who had complete regression of the primary tumor at cervix along with smoothening of both parametrium were considered as complete response (CR) while all others were taken as partial response (PR). Patients who continued to have no evidence of any loco-regional disease and on follow-up were considered as censored for the purpose of survival analysis. Toxicity scoring was done as per RTOG/ EORTC criteria.12 Dose-regression curves were plotted individually for each of the 77 patients taking into account the percentage responses achieved at the corresponding EXTRT dose while on treatment. The scatter plots were fitted (cubic fit) and various parameters for the curve TRD50, TRD80, g50, slope50 and q50 were estimated directly from the curve. TRD50 and TRD80 represent the tumor control doses (TRD) (in Gy) for a 50% and 80% response respectively. The normalized dose gradient- g50, expressed as %/%, was the increment in response, in percentage points for a 1% increase in dose, defined at the 50% response level.4,5 Slope50, was estimated from the relation, Slope50 (%/Gy) = 100 (g50/ TRD50).3 The other proposed measure of the slope of the dose-response curve - q50, was calculated using the relation, q50 (%/Gy) = g50 / TRD50.7 Off the 77 patients included in this study, in 3 patients, the above parameters could not be quantified since the total gross response at end of EXTRT failed to reach 50%. Response status at completion of EXTRT and ICBT were assessed for demographic parameters using either a chi-square or student's "t test". The impact of various individual dose-response curve parameters - TRD50, TRD80, g50, slope50 and q50 for the patient and treatment related variables were evaluated. The normality tests for these variables were tested using Kolmogorov Smirnov test.13 The means of these values for patient and treatment variables were tested using "t test" for univariate analysis. For gross features these were tested using one way ANOVA. Kaplan-Meier estimates were computed for patients with AGRT for loco-regional disease free survival (LDFS).14 Survival analysis was based on worst case scenario. Multivariate analysis using Cox's proportional hazard model was also performed to look for the dose-response variables likely to significantly influence the LDFS.15 For both logistic regression and Cox's proportional hazard model, various dose-response variables were entered using a forward step wise regression with probability of F to enter being <0.05 and removal at > 1.0. The factors entered into regression model were - TRD50, TRD80, g50, slope50 and q50. The exponent of coefficient b and its 95% confidence intervals were computed. All the statistical calculations were performed using SPSS software package for windows, version 9.0 (SPSS Inc. Chicago, IL, USA). RESULTS For maintaining a uniform cohort of patients for this study, all the 77 patients evaluated had received an identical dose and fractionation schedule of EXTRT and ICRT. Age ranged from 27 to 77 years (median: 50 years) and except 2 patients, all had squamous cell carcinoma. Most of them were either in FIGO stages II or III and had ulceroproliferative tumors. Pretreatment hemoglobin at presentation, ranged from 6.4 gm% to 14 gm%. Every effort was made to ensure that before start of radiotherapy, hemoglobin was at least 10 gm% or more by blood transfusions and iron supplementations. Although all the patients had received 50 Gy of EXTRT at 2 Gy per fraction, overall treatment time for EXTRT ranged from 33 to 52 days. The detail demographic features are listed in Table 1. Fifty-three patients (68.8%) had achieved a CR at one month following the end of EXTRT and ICBT. Of these, 40 (51.9%) had AGRT at completion of EXTRT alone. Significantly severe (> grade 3) acute bladder and rectal toxicity was experienced by 1 and 3 patients respectively. Only two patients reported with grade III late bladder morbidity, while none had similar late rectal toxicity. Univariate analysis revealed that younger patients (< 50 years) were more likely to have residual disease at one month from completion of radiotherapy (P=0.052). No other factors like gross features, FIGO stages, pre-treatment hemoglobin, histology or overall EXTRT treatment time within the range in which this was delivered had any significant impact on the likelihood of a CR at end of radiotherapy (Table 2). The maximum follow up period was 71 months and the cumulative probability of LDFS at 5 years was estimated at 36% (median: 34 months). There was strong evidence that patients who had an absence of gross residual tumor at completion of EXTRT had a greater probability of achieving a better LDFS (P=0.046, Figure 1). Additional quantum of response to brachytherapy was not found to be different between those with CR and PR at end of the entire course of radiotherapy, median being 10% and 12.5% respectively. Apart from tumor response at completion of EXTRT (AGRT or PGRT) and at 1 month of completion of radiotherapy (CR or PR), none of the patient demographical parameters nor duration of treatment was found to have an impact on LDFS (Table 3). The various parameters for quantifying the position and slope of the dose response curves were directly read from curve fits of individual patients. TRD50, TRD80, g50 values were normally distributed while slope50 and q50 had a significance value which was at the lower bound of significance. The interquartile range for slope50 and q50 are 0.819 and 0.008 respectively. The fitted dose-response curve for all the 77 patients during EXTRT was sigmoid. Addition of ICBT did not change the shape or position of this curve, except stretching the terminal plateau segment. Curve fits were generated from the scatter plots of dose-response separately between patients based on known prognostic factors, which could have an impact on the outcome. These include age, FIGO stage, gross features, pretreatment hemoglobin, EXTRT treatment time and response with EXTRT (Figure 2). Of these, the curves for age groups, FIGO stage groups and responders with EXTRT were different in terms of the slope and their positions. These were also evident from the significant differences in the estimated parameters of the tumor regression parameters namely TRD50 (P=0.049) and TRD80 (P=0.049) for age groups; TRD80 (P=0.050) and slope50 (P=0.008) for FIGO stage group and TRD50 (P<0.001), TRD80 (P<0.001), and slope50 (P=0.001) for responders to EXTRT (Table 4). The curve was shifted to the right for the poor prognostic groups, while in all other cases; curves almost superimposed or crossed over at some points. On logistic regression for AGRT versus PGRT at end of EXTRT, only TRD50 (P=0.017) and TRD80 (P=0.004) retained their significance (Table 5). However, of all the EXTRT dose-regression parameters evaluated, only TRD80 was found to influence LDFS on multivariate analysis (Table 5). DISCUSSION The present study attempted to identify the prognostic variables for different endpoints and correlate them with radiation dose-response characteristics. With a uniform dose of radiotherapy to all patients, age and quantum of regression achieved during EXTRT were found to impact the loco-regional control and LDFS. Similar observations have been reported by others.10,11,16 Dose-response relationship has been previously studied for a wide range of tumors where loco-regional controls at completion of various dose schedules have been presented.1-3 In the present study, responses occurring over the entire range of dose delivered have been considered. The responses recorded could have an element of subjectivity since these were based on clinical examination alone. However, even radiological assessment and estimation of volumes of the primary tumor during EXTRT at the cervix and parametrium, could be ambiguious.17 Moreover, it would not be practically possible to undertake weekly radiological assessments in the routine set up of a department and also not financially feasible for patients to pay for weekly radiological studies involving either computed tomography or magnetic resonance imaging. Nevertheless, the relation obtained by clinical examination was a sigmoid curve, which is widely accepted to represent the radiation dose-response relationship. Different authors have argued and tried to justify the various parameters that would give a true representation of the "S" shaped curve in terms of its position and steepness.3-5,7 In view of such uncertainties; the estimates of the various parameters in this study were made directly from the graphs based on their definitions. Okunieff et al. had estimated the TRD50, g50, and slope50 of carcinoma of the cervix from the literature and reported to vary from 24.27 to 64.38 Gy, 0.64 to 20.93 %/% and 1.08 to 61.27%/Gy respectively.3 On excluding the outliers from the estimates of stages IIB and III (from Perez et al.18 and Perez and Kao19) values for TRD50, g50and slope50 in carcinoma of the cervix ranged between 24 - 34Gy, 0.64 0.71 %/% and 2.52 2.77 %/Gy respectively. The mean TRD50, g50, and slope50 values for the entire group of our patients has been 34.68 Gy, 0.77 %/% and 2.24 %/Gy respectively. These are in close agreement with those estimated by Okunieff et al.3 These values were different for different subgroups and between the responders and nonresponders as listed in Table 4. Thus, of all the parameters evaluated in this study, position and steepness of the dose-response curves are best represented by TRD80 which is also reflected in multivariate analysis for LDFS (Table 5). Since TRD80 has been observed to be the most significant parameter in this study, other variables have been compared with TRD80. A closer perusal indicates that patients with AGRT following EXTRT had a less scatter of various parameters compared to those with PGRT (Figure 3). This could indicate a greater degree of heterogeneity in partial responders in terms of their biological behavior and could contribute to a relatively inherent radioresistance to conventional radiation therapy. For all patients, TRD50 and TRD80 show a linear positive correlation, with patients having AGRT clustered at the lower values of TRD80 (Figure 3a). g50 did not follow an expected pattern of fall with increasing TRD80 (Figure 3b). This could be explained by the non significant difference in g50 values between AGRT and PGRT patients (Table 4). Slope50 and q50 demonstrated a gradual decline with increase in TRD80 (Figures 3c and 3d). The parameters of slope50 and q50 differ only by a factor of 100 and hence have a perfect linear relation between them (Figure 3e). The slope50 and g50, both of which indicate the steepness of the dose-response curve, also exhibit a linear relation. However, patients with AGRT have a higher slope50 value compared to those with PGRT for any g50value (Figure 3f). It thus appears that there could be certain subsets of patients who might fail to conventional radiotherapy and might be benefited by concomitant chemoradiotherapy. These could be patients younger than 50 years and those with tumors which are inherently radioresistant.20-22 These could be identified by various tumor cytokinetic studies and radiobiological parameters.23-25 Thus, even with the gradual acceptance of chemotherapy as a part of treatment protocol for cancer cervix, it could be important to identify certain subsets of patients who would be benefited with the addition of chemotherapy.26-29 With a planned combination of EXTRT and ICBT, a 5 year survival ranging from 62% to 78% in stages I and II and 43% to 50% in stages III have been reported even from developing countries, like India.30 Moreover, as the recent phase III trial31 between radiotherapy alone versus chemoradiotherapy in cancer cervix has failed to show any benefit with chemotherapy, therapeutic options should be carefully weighed. Till results from further large sample stratified randomized trials based on the possible prognosticators are available, acute and long term toxicities that could result following chemoradiotherapy should influence therapeutic decisons.32 This could be of importance in developing countries where loco-regional advanced cancer cervix is a major cancer problem, especially for the weaker socio-economic class of population. REFERENCES
Copyright 2004 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn04004t4.jpg] [cn04004f1.jpg] [cn04004f3.jpg] [cn04004t2.jpg] [cn04004f2.jpg] [cn04004t3.jpg] [cn04004t5.jpg] [cn04004t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}