 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 41, No. 1, (January-March 2004) , pp. 25-31 Alterations in plasma lipid profile patterns in head and Neck Cancer and Oral Precancerous Conditions Patel PS, Shah MH, Jha FP, Raval GN, Rawal RM, Patel MM, Patel JB, Patel DD Biochemistry Research Division, Department of Cancer Biology; The Gujarat
Cancer & Research Institute, Asarwa, Ahmedabad - 380016, India.
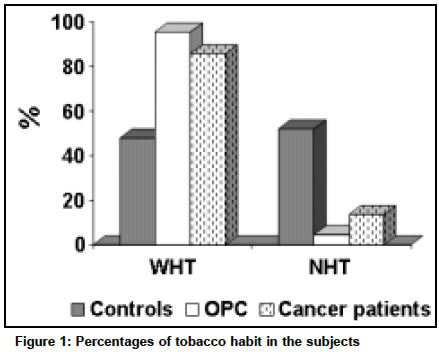
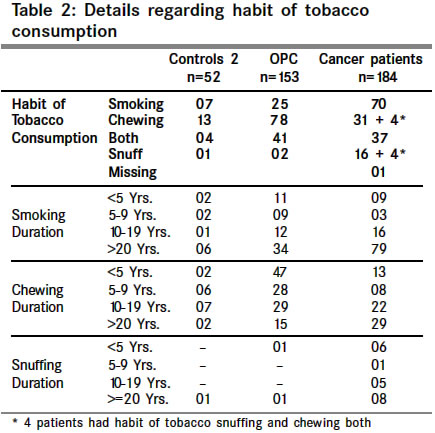
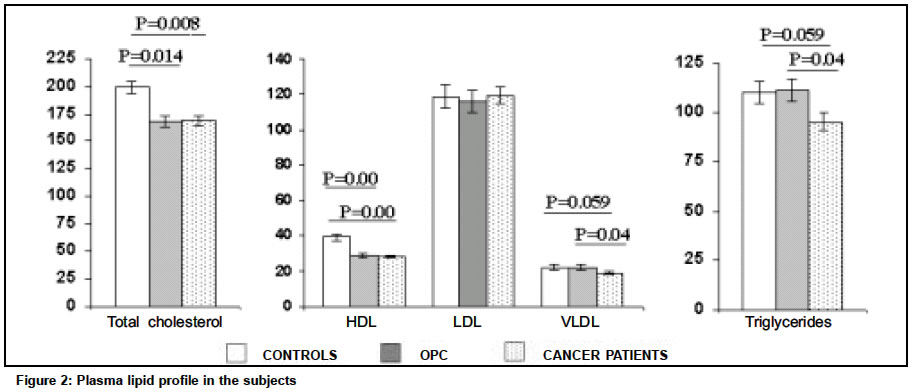
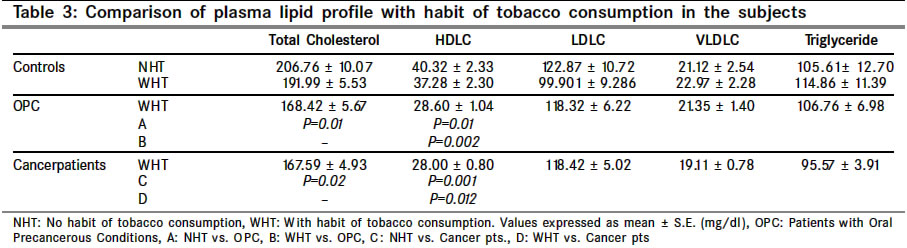
Code Number: cn04005 ABSTRACT BACKGROUND: The changes in lipid profile have long been associated with cancer because lipids play a key role in maintenance of cell integrity. AIMS: The present study evaluated alterations in plasma lipid profile in untreated head and neck cancer patients as well as patients with oral precancerous conditions (OPC) and its association with habit of tobacco consumption. MATERIAL AND METHODS:This hospital-based case control study included 184 head and neck cancer patients, 153 patients with OPC and 52 controls. Plasma lipids including: (i) Total cholesterol, (ii) LDL cholesterol (LDLC), (iii) HDL cholesterol (HDLC) (iv) VLDL cholesterol (VLDLC) and (v) triglycerides were analysed by spectrophotometric kits. STATISTICAL ANALYSIS USED: Student's t-test was performed to compare mean values of the parameters. RESULTS: A significant decrease in plasma total cholesterol and HDLC was observed in cancer patients (p=0.008 and p=0.000 respectively) as well as in patients with OPC (P=0.014 and P=0.000, respectively) as compared to the controls. The plasma VLDL and triglycerides levels were significantly lower in cancer patients as compared to the patients with OPC (P=0.04) and controls (P=0.059). The tobacco habituates showed lower plasma lipid levels than the non-habituates. Our data strengthen the evidence of an inverse relationship between plasma lipid levels and head and neck malignancies as well as OPC. CONCLUSION:The lower levels of plasma cholesterol and other lipid constituents in patients might be due to their increased utilization by neoplastic cells for new membrane biogenesis. The findings strongly warrant an in-depth study of alterations in plasma lipid profile in head neck cancer patients. Key Words: Lipids, Cholesterol, Triglycerides, Head and neck cancer, Oral precancerous conditions. INTRODUCTION Lipids are major cell membrane components essential for various biological functions including cell growth and division of normal and malignant tissues. Usefulness of variations in tissue/blood cholesterol levels in diagnosis and treatment of various diseases has been studied by several workers. Although, its prime role in pathogenesis of coronary heart disease has been consistently found, researchers have reported association of plasma/serum lipids and lipoproteins with different cancers.1-4 The alterations in the circulatory cholesterol levels have been found to be associated with etiology of breast cancer and colorectal cancer.5-7 However, only a few reports are available on plasma lipid profile in head and neck cancer.1,8 Head and neck cancer is one of the leading causes of morbidity and mortality due to cancer. Its incidence is much higher in Asian countries, as compared to the West. At our Institute (The Gujarat Cancer and Research Institute), head and neck cancer accounts for about 2300 new cases every year which is around 25.3% of all cancer cases.9 The habit of tobacco consumption is a known etiologic factor for development of oral precancerous diseases and head and neck cancer.10,11 Patients with oral precancerous conditions (OPC) have also been reported to show a significant tendency to develop cancer.12 It is believed that tobacco carcinogens induce generation of free radicals and reactive oxygen species, which are responsible for high rate of oxidation/peroxidation of polyunsaturated fatty acids. This peroxidation further releases peroxide radicals. This affects essential constituents of the cell membrane and might be involved in carcinogenesis/tumorigenesis.13 Because of the lipid peroxidation, there is a greater utilization of lipids including total cholesterol, lipoproteins and triglycerides for new membrane biogenesis. Cells fulfill these requirements either from circulation, by synthesis through the metabolism or from degradation of major lipoprotein fractions like VLDL, LDL or HDL. Earlier reports have shown that antioxidant vitamins have protective effects against lipid peroxidation.14-16 Lower blood lipids have been associated with various cancers.2,4,17,18 Furthermore, some investigators have also found relation of low serum cholesterol with increased risk of cancer occurrence19,20 and mortality.21,22 The plasma concentrations of lipids are not the single additive function of intake, utilization and biosynthesis because of its continuous cycling in and out of the blood stream. The question that whether hypolipidemia at the time of diagnosis, is a causative factor or is a result of cancer has remained unanswered. Considering these curiosities, the present study was aimed to evaluate the plasma lipid profile including: (i) total cholesterol, (ii) LDL cholesterol (LDLC), (iii) HDL cholesterol (HDLC), (iv) VLDL cholesterol (VLDLC) and (v) triglycerides in head and neck cancer patients, patients with OPC and healthy individuals. The association between alterations in plasma lipid profile and habit of tobacco consumption was also studied. MATERIAL AND METHODS Subjects Fifty-two healthy individuals, who had no complaint or any major illness in recent past, were included in the study as controls. They were close relatives of the patients accompanying them during their hospitalization. One hundred fifty three patients with OPC were also included in the study from the Government Dental College and Hospital, Civil Hospital Campus, Ahmedabad. Out of these, 97 (63.4%) had oral submucous fibrosis, 44 (28.8%) had oral leukoplakia and 12 (7.8%) were with other diseases including dysplasia and verrucous hyperplasia. The hospital-based case control study included 184 untreated head and neck cancer patients, enrolled from the outpatients' department of the Gujarat Cancer and Research Institute, Ahmedabad. The patients were diagnosed as having cancer of oral cavity (n=121), pharynx (n=49), larynx (n=10) and maxilla (n=4). The diagnosis was based on clinical and histopathological examinations. Staging was done according to UICC classification.23 Table 1 provides clinicopathological details of cancer patients. Histologically, 174 (94.6%) patients represented with squamous cell carcinoma. Twenty-eight patients had early disease (stage I and II) and 131 had advanced disease (stage III and IV). The classification according to their histological grade revealed that 64 patients had well differentiated, 85 had moderately differentiated, 20 had poorly differentiated and 5 had undifferentiated carcinoma. The subjects in each group were further classified into as having no habit of tobacco consumption (NHT) and with habit of tobacco consumption (WHT). Blood sample collection Fasting blood samples were collected from the subjects, into EDTA containing vacuettes. Samples were centrifuged; plasma was collected and stored at 800C until analyzed. METHODS Plasma cholesterol levels were estimated using cholesterol kits obtained from Autospan Reagents, Span Diagnostics (Gujarat, India). Briefly, 5 µl of plasma sample was mixed with 500 µl of working reagent that contained cholesterol oxidase, cholesterol esterase, peroxidase, 4-amino phenanzone, surfactant, phenol, buffer, preservatives and stabilizer. The mixture was incubated at 370C for 10 minutes and absorbance was read at 505 nm. Plasma HDL cholesterol levels were also estimated using Autospan kits obtained from Span diagnostics (Gujarat, India). Briefly, 0.3 ml plasma sample was mixed with 0.3 ml precipitating reagent (PEG 6000, stabilizer and preservative), followed by 10 minutes incubation at room temperature. The mixture was centrifuged at 2000 rpm for 15 minutes. The supernatant obtained was mixed with working cholesterol reagent. After incubation of 10 minutes at 370C, absorbance was read at 505 nm. The triglyceride levels were estimated using liquid gold kits, obtained from Autospan reagents, Span diagnostics (Gujarat, India). Briefly, 10 µl plasma sample was mixed with 1000 µl of triglycerides assay reagent containing Pipes buffer, lipase, 4chlorophenol, Magnesium ion, ATP, lipase, peroxidase, glycerol kinase, sodium azide, 4amino antipyrene, glycerol-3-phosphate oxidase and detergents. The mixture was then incubated for 10 minutes at 370C and absorbance was read at 505 nm. VLDLC and LDLC levels were calculated as shown below: VLDLC = Triglycerides/5 LDLC = Total Cholesterol (VLDLC) (HDLC) STATISTICAL ANALYSIS Student's t-test was performed to compare mean values of the parameters. "P" value <0.05 was considered to be statistically significant. Results Habit of tobacco consumption in the subjects Habit of tobacco consumption in one or the other form (smoking/chewing/snuff) is highly prevalent in this region. As depicted in Figure 1, 95.4% of the patients with OPC and 85.8% of the cancer patients were consuming tobacco in one or the other form. The details regarding habit of tobacco consumption are provided in Table 2. Tobacco chewing in the form of readily available pouch (gutkha) and/or with lime was common in the patients with OPC and bidi (country cigarette) smoking among the cancer patients. Habit of tobacco snuff (oral/nasal) was usually observed in the female subjects, especially in female cancer patients. Use of tobacco, on an average, was greater than 10 years in all the subjects. 79/107 (73.8%) of the smokers in cancer patients and 34/66 (51.5%) of the smokers in patients with OPC had habit of smoking for more than 20 years. While, 29/72 (40.3%) of the tobacco chewers in cancer patients had habit of chewing for more than 20 years. Plasma lipid profile in the patients at the time of diagnosis The mean plasma lipid profile of controls and patients, at the time of diagnosis, are represented in Figure 2. A significant decrease in plasma total cholesterol and HDLC were observed in cancer patients (P=0.008 and P=0.000, respectively) as well as in patients with OPC (P=0.014 and P=0.000, respectively) as compared to the controls. However, the mean plasma levels of total cholesterol and HDLC were comparable between patients with OPC and cancer patients. The VLDLC and triglycerides levels were lower in cancer patients as compared to the controls (P=0.059) as well as the patients with OPC (0.04). However, plasma levels of VLDLC and triglycerides were comparable between controls and patients with OPC. Plasma LDLC levels did not reveal any significant difference among all three groups. Plasma lipid status in NHT and WHT subjects Further, we compared plasma lipid levels between NHT and WHT subjects (Table 3). First, the plasma lipid levels between tobacco consumers and non-consumers of the control group were compared. The controls consuming tobacco showed lower mean plasma lipid levels than the non-consumers. Secondly, the plasma lipid levels in tobacco habituates with OPC and cancer were also compared with the controls. Total cholesterol levels were significantly lower in WHT subjects with cancer (P=0.02) and OPC (P=0.01) as compared to the NHT. Likewise, HDLC levels were decreased in WHT subjects with cancer (P=0.001) and OPC (P=0.01) as compared to the NHT. Significantly low level of HDLC in patients with OPC and cancer patients as compared to controls (both NHT and WHT) (Table 3). When subjects were further categorized into above and below cutoff level (considering median of NHT as cut off), it was found that greater proportion of the subjects with OPC and cancer were having total cholesterol, HDLC,VLDLC and triglyceride levels below cutoff limit (Figure 3) DISCUSSION Cholesterol and triglycerides, important lipid constituents of cell, are essential to carry out several vital physiological functions. Cholesterol is essential for maintenance of the structural and functional integrity of all biological membranes. It is also involved in the activity of membrane bound enzymes and is important for stabilization of DNA helix.24 Cellular uptake and regulation of cholesterol is mediated by lipoprotein receptors especially located on the surface of the cells. For transport in plasma, triglycerides and cholesterol are packaged into lipoproteins, which are then taken up and degraded by cells to fulfill demands for cellular functions. In some malignant diseases, blood cholesterol undergoes early and significant changes. Low levels of cholesterol in the proliferating tissues and in blood compartments could be due to the process of carcinogenesis. The question arises whether hypolipidemia is a predisposing factor or result of cancer? However, earlier studies have reported that hypolipidemia may result due to the direct lipid lowering effect of tumor cells or some secondary malfunction of the lipid metabolism or secondary to antioxidant vitamins.21,25-29 Several prospective and retrospective studies have shown an inverse association between blood lipid profile and different cancers.2,4,17,18,30 Schatzkin et al1 and Chyou et al8 have observed an inverse trend between lower serum cholesterol and head neck as well as esophageal cancers. The results are strengthened by the present study showing lower plasma total cholesterol, HDLC, VLDLC and triglycerides in head and neck cancer patients and patients with OPC than the healthy individuals. Cholesterol is an essential constituent of lipoprotein fractions like LDL, HDL and VLDL. Seventy five percent of the plasma cholesterol is transported in the form of LDLC. Body cells sequester cholesterol from LDL fraction of lipoproteins. LDL receptors are necessary for metabolizing circulating LDLC levels and nearly 80% of the plasma LDLC is cleared by LDL receptors.31 High activity of LDL receptors attributes for lowering the serum cholesterol levels. The individuals having deficient or defective LDL receptors remove plasma LDLC at much lower rate and have considerably elevated levels.32 In the present study, a significant decrease was observed in plasma HDLC in cancer patients. This is in accordance with previous reports, that low HDLC is an additional predictor of cancer2,30,33 and it might be a consequence of disease that is mediated by utilization of cholesterol for membrane biogenesis. We observed significantly decreased VLDLC and triglyceride levels in cancer patients as compared to the controls and patients with OPC. Alexopoulos et al18 have found non-significant difference in serum triglycerides between controls and patients. While others have observed elevated triglycerides levels in cancer patients.2,34 Lipid peroxidation is an essential biochemical process that involves the oxidation of polyunsaturated fatty acids, the important components of cell membranes. Tobacco carcinogens generate reactive oxygen species and lipid peroxides, leading to tissue injury due to elevated lipid peroxidation, further damaging the cellular structural blocks like lipids, proteins, DNA etc. Thus, lipid peroxidation may play a role in endogenous formation of exocyclic DNA adducts. In our study, about 95% of the patients with OPC and 85% of the cancer patients were tobacco consumers. Therefore, levels of the lipids in WHT subjects in patients with OPC and cancer patients were compared with plasma lipid profile of NHT group of controls. Higher plasma cholesterol, HDLC, VLDLC and triglycerides were observed in controls without habit of tobacco consumption than controls and patients with tobacco habits. Earlier studies have shown an inverse relation between cholesterol and tobacco related cancers.1,20 Neufeld et al35 have reported passive smoking as a significant risk factor for decreased HDLC. Animal studies have shown that nicotine, a known tobacco carcinogen, affects activity of enzymes responsible for lipid metabolism.36 It is also reported that LDLC uptake and cholesterol biosynthesis were decreased in the liver of tumor bearing animals.23 Further, exposure to tobacco carcinogens hampers antioxidant defense, leading to accelerated lipid peroxidation. There is a strong relationship between vitamin E (a liposoluble antioxidant vitamin) and lipids, especially cholesterol. Vitamin E is co-transported with all forms of cholesterol and contributes to the first line of defense against lipid peroxidation.14 Further, triglycerides and cholesterol are positively correlated with vitamins.37 We observed a significant decrease in plasma levels of fat-soluble antioxidant vitamins such as vitamin E and b-carotene in tobacco habitués.38 Together, our study shows declined plasma levels of total cholesterol, HDLC, LDLC, VLDLC and triglycerides. As majority of the patients with OPC and cancer patients were with habit of tobacco, marker levels in NHT controls were compared with WHT controls, patients with OPC and cancer patients with habit of tobacco to eliminate any bias due to tobacco habit. To establish a cutoff of circulating marker level equal numbers of controls with and without habit of tobacco were enrolled. From the present study we can't predict the incidence of tobacco habitués in healthy population. In conclusion, Rose et al39 reported 66% higher mortality rate due to cancer in the group of cancer patients with lowest plasma cholesterol than in the highest plasma cholesterol. Our results add to this evidence of an inverse relationship between lower plasma lipid profile and head and neck malignancies and oral precancerous conditions. The lower plasma lipid status may be a useful indicator for initial changes occurring in neoplastic cells. However, a detailed study of cholesterol carrying lipoprotein transport and the efficiency of the receptor system may help in understanding the underlying mechanisms of regulation of plasma cholesterol concentrations in cancer. Further work on these interesting results as well as in-depth studies on lipoprotein transport and receptor system is in progress in our laboratory. ACKNOWLEDGEMENTS The authors are sincerely thankful to Cancer Treatment Research Foundation, Washington, D.C., USA, for providing financial support (Grant No. G96134) for this study. REFERENCES
Copyright 2004 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn04005f2.jpg] [cn04005t3.jpg] [cn04005t1.jpg] [cn04005t2.jpg] [cn04005f1.jpg] [cn04005f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}