 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 41, No. 1, (January-March 2004) , pp. 41-46 Case Report Gangliogliomas: A Report of Five Cases Nair V, Suri VS, Tatke M, Saran RK, Malhotra V, Singh D* Departments of Pathology and *Neurosurgery, G. B. Pant Hospital, New Delhi,
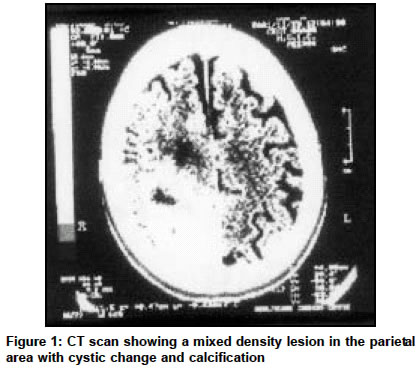
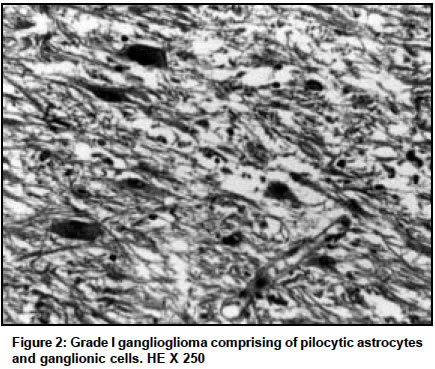
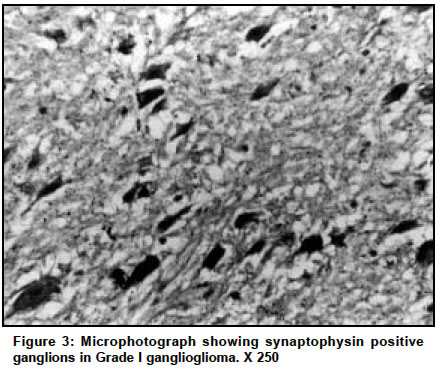
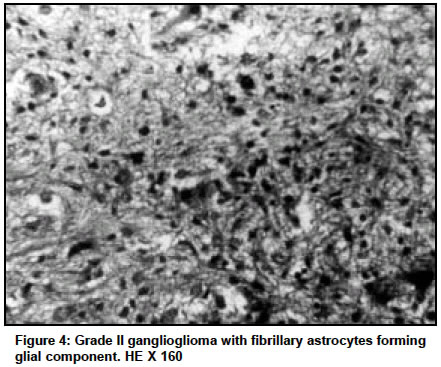
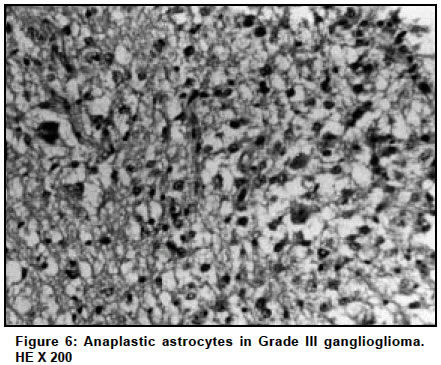
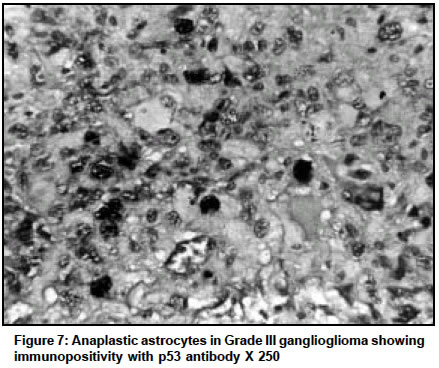
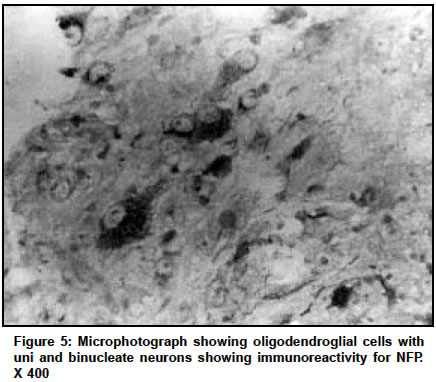
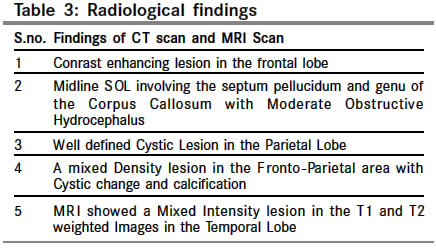
India. Code Number: cn04008 ABSTRACT Gangliogliomas are rare tumors of the Central Nervous System. Five Gangliogliomas were diagnosed out of 1560 brain tumours surgically resected out in a period of 5years accounting for 0. 32%. We have tried to discuss in detail the pathological features of these tumours and have mentioned the clinical and radiological features associated with them. All the slides, tissue blocks and pathology reports of the surgical specimens of gangliglioma were reviewed and the clinical and radiological data reviewed. The ages of the patients ranged from 7 - 65 years with 4 males and 1 female. The tumors were located in the lateral ventricle (a rare site), temporal, parietal and the frontal lobes with duration of seizures varying from 1- 9 years. The tumors were diagnosed by the presence of a dual population of neoplastic ganglionic and glial components. The glial components consisted of pilocytic astrocytes (l case), fibrillary astrocytes (2 cases), oligodendrocytes (1 case) and anaplastic astrocytes and oligodendrocytes (1 case). There was one-grade I GG, three-Grade II GGs and one-grade III GG. Astrocytes were the commonest glial component of GGs, either pilocytic or fibrillary. Oligodendrocytes as the glial component of GGs was seen in 2 cases one of which was anaplastic and this is a rare finding. Key Words: Ganglioglioma, Anaplastic Gangliogliomas. INTRODUCTION Gangliogliomas are rare central nervous tumors composed of intimately admixed neuronal and glial components and account for approximately 2% of all brain tumors. Though these tumours are rare they have a benign biological behavior and hence it is important to make an accurate diagnosis. In this study we have retrieved 5cases out of the 1560 cases of central nervous system diagnosed for the past 5 years in our department. We have discussed in detail the histopathological criteria and characteristics of these tumors in great detail and also included the clinical and radiological features associated with these tumours. Case Reports (Table 1) All the slides, tissue blocks and pathology reports of surgical specimens from patients with ganglioglioma operated between 1998 to 2002 were retrieved from the files of the department of pathology. There were a total of 1560 cases of brain tumours, out of which five cases were that of Gangliogliomas. All the cases were reviewed and analyzed retrospectively. All specimens had been fixed in formalin and processed for paraffin embedded sections. Hematoxylin and eosin staining was done in all cases. Immunohistochemistry was done, using antibodies to glial fibrillary acidic protein (GFAP), synaptophysin, neurofilament protein (NFP), vimentin, S 100 protein, p - 53 and MIB - 1 (all from DAKO Carpinteria, CA) by the labelled Streptavidin - Biotin technique. The microscopic criteria for the diagnosis of ganglioglioma were considered if the tumor was composed of mixture of glial cells and neurons. (a) They were recognized as neurons if the cells were large with vesicular nuclei and prominent nucleoli. and if they stained positive for synaptophysin or neurofilament protein. (b) the glial cells were recognized as astrocytes if they showed cytoplasmic staining for GFAP and oligodendrocytes if they showed perinuclear staining for GFAP. The glial component of all the cases were reviewed for pleomorphism, tumor giant cells and mitosis and considered anaplastic if these features were present. The ganglioglioma in which the glial component was formed of pilocytic astrocytes was considered Grade I, while those whose glial component was composed of fibrillary and oligodendroglial component with no pleomorphism, mitoses or tumour giant cells were considered Grade II. If the astrocytic or oligodendroglial component showed pleomorphism, mitoses and tumour giant cells, it was diagnosed as Grade III. The corresponding clinical charts and all available CT and MRI scan findings of the cases from the clinical department of Neurosurgery were reviewed. Case 1 A 7-year-old boy presented with complaint of seizures mainly involving the left half of the body for the past 6 years. CT scan showed a contrast enhancing lesion in the right frontal lobe in the region of the caudate nucleus. A right fronto temporal craniotomy with decompression of the mass was done. The tissue was sent for histopathological examination. Case 2 A 65-year-old female presented with headache on and off for a period of 6 months and weakness of the right lower limb for 10 days. CT scan showed an anterior midline space occupying lesion (SOL) involving the septum pellucidum and genu of corpus callosum with obstruction and moderate hydrocephalus. A provisional clinical diagnosis of malignant glioma was made. Left frontal craniotomy with tumour decompression was done and tissue sent for histopathological examination. Case 3 A 21-year-old male presented with seizures for past 3 1/2 years. The seizures were generalised involving all 4 limbs. CT scan showed a well defined cystic lesion in the left parietal lobe. On MRI-T 1 images showed hypointense lesion in the left parietal area with well defined margins. The T2 images showed a hyperintense lesion in the left parietal area with well defined margins. The differential diagnosis were - cystic glioma and hydatid cyst. Left parietal craniotomy with excision of cyst was done and tissue sent for histopathology. Case 4 A 60-year-old male presented with complaints of seizures with weakness of the body for past 1 year. CT scan showed a mixed density lesion in the right parietal area with cystic change and focal calcification (Figure 1). Right parietal craniotomy with decompression was done and tissue sent for histopathology. Case 5 A 16-year-old male presented with intractable seizures since the age of 7 years. MRI showed a mixed intensity lesion in T I and T2 weighted images, in the temporal lobe. A provisional clinical diagnosis of glioma was made. Right temporal craniotomy and decompression of the mass was done and tissue sent for histopathology. DISCUSSION In case 1, there was large number of pilocytic astrocytes (Figure 2) along with interspersed Rosenthal fibers. Admixed among these were large cells with vesicular nuclei and prominent nucleoli. These cells showed variation in size and shape and lack of orientation. A diagnosis of ganglioglioma was made. Immuno-histochemistry was done to confirm this. The pilocytic astrocytes and Rosenthal fibers showed cytoplasmic positivity for GFAP and the ganglion cells were immunoreactive for synaptophysin (Figure 3). In case 2 and 3 the tumor was composed of fibrillary astrocytes (Figure 4). Besides these, there were few isolated large cells with abundant eosinophilic cytoplasm and vesicular nuclei with prominent nucleoli. Possibilities of glioma and ganglioglioma were considered. Immunohistochemistry was done and the fibrillary astrocytes were immunoreactive for GFAP while the larger cells showed immunoreactivity for NFP. MIB-1 labeling index was < 1% and occasional nuclei showed p 53 positivity, thus confirming the diagnosis of ganglioglioma. In case 4, there was a polymorphous population of cells. There were astrocytes which showed pleomorphism, tumor giant cells and mitosis indicating these were anaplastic (Figure 6). In addition, there was a considerable population oligodendroglial cells and a third population of neuronal cells. Immunohistochemistry was done. The anaplastic astrocytes showed cytoplasmic positivity for GFAP while the oligodendroglial cells showed perinuclear and cytoplasmic positivity for GFAP nuclear immunoreactivity for S-100 protein. The neuronal cells were immunoreactive for NFP (Figure 8) and Synaptophysin. The MIB-1 labeling index was 6%, and 8% of the nuclei showed p 53 positivity (Figure 7) In case 5, the tumor was composed of oligodendroglia cells with vesicular nucleus with perinuclear clearing. Occasional mitosis was noted. Admixed amongst these were neuronal cells with vesicular nucleus, prominent nucleoli and abundant cytoplasm. A diagnosis of ganglioglioma was considered. Immunohistochemistry was done. The oligodendroglial cells were not immunoreactive for GFAP but were immunoreactive for S-100. The larger cells were immunoreactive for NFP (Figure 5) and synaptophysin. The MIB- I labelling index was 2%. There was no p 53 positivity in this tumor. All cases showed perivascular lymphocytes and calcification. Cases 1, 3 , 4 and 5 were present in the white matter of lobes and case 2 was intraventricular. There was one case of Grade I ganglioglioma (case 1), three cases of Grade II ganglioglioma (case 2, 3 and 5) and one case of Grade III ganglioglioma (case 4), in which the glial component was mixed oligoastrocytic (Table 2). The term ganglioglioma was introduced by Courville in 1930 to describe a tumor in which mature neuroglia co-existed with ganglion cells.2 The tumors account for approximately 2% of all brain tumours.1 In our study we had 5 cases out of 1560 of central nervous system over a span of 5 years making an incidence of 0. 32%. The age of presentation is generally the first decade of life.1 In our study the ages ranged from 7 years to 65 years with a mean of (32 years) as compared to the study Uma. P. Kalyan et al in which the mean age was 34.3 years.4 In our study there was a male preponderance, with four out of five cases being males. Although the most frequent intracranial location of the ganglioglioma is the temporal lobe, other locations in order of frequency include frontal, parietal and occipital lobes.8 Brain stem and spinal cord are also involved.9 Intraventricular location is rare for gangliogliomas.3 In our series 2 cases were situated in the parietal lobe, one is the frontal lobe and one in the temporal lobe. We had one case of ganglioglioma located in the lateral ventricle (case 2). The most common presenting symptom is seizures.10 In our series 4 out of 5 cases presented with seizures. In our study the duration of the seizures ranged from 6 months to 6 years. In a clinico-pathological and radiological study by Dr. Uma P. Kalyan, CT scan showed a low density enhancing mass in 80% and calcification in 50% of cases.4 In our study 2 cases on CT scan showed a contrast enhancing lesion. In one case the CT scan showed a well defined cystic lesion while in other it showed a mixed density lesion with cystic change. In the fifth case MRI was done which showed a mixed intensity lesion in the T1 and T2 weighted Images, In our series Calcification was seen in all the cases. (Table 3). Macroscopically, gangliogliomas are usually well circumscribed firm masses with a granular appearance on cut section.11 The microscopic criteria for the diagnosis of ganglioglioma was given by Russell and Rubenstein which are as follows - (a) the tumor is composed of mixture of glial cells and neurons, (b) the glial cells consist mostly of astrocytes, (c) the cells are identified as neurons only if Nissl substance can be demonstrated by cresyl violet stain or if they give origin to neuronal processes, demonstrated by modified Bielschowski or Bodian stain.12
The criteria for the diagnosis of neoplastic neurons are: a) histologically- the neurons are in heterotopic locations as in the white matter, subarachnoid space and in the ventricles. b) Biologically- the ganglion cells are in irregular groups with transitional forms. c) Cytological- the neurons are bizarre, dysmorphic, varying in size and shape with abnormal orientation of axonal and dendritic processes and binucleate forms.13 In the present study in all the cases these were cytologicaly dysmorphic with lack of orientation. According to the 1993 WHO classification, gangliogliomas are graded as Grade I and II and anaplastic gangliogliomas as Grade III.5 The glial component of a ganglioglioma is usually composed of low grade astrocytes fibrillary or Pilocytic but cases with oligodendroglial component have also been reported.6 In our study 2 cases had fibrillary astrocytes as the glial component and 1 had pilocytic astrocytes. We had one case with oligodendroglial cells forming the glial component. Ependymoma forming the glial component has been recently described.7 The glial component can also have anaplastic feature [10]. In our study we had one case in which the glial component was composed of anaplastic astrocytic and oligodendroglial cells. There is a case report of transformation of a Grade I ganglioglioma into a Grade II ganglioglioma in the first recurrence and into a Grade IV glioblastoma in the second recurrence.14 On molecular genetic analysis a Tp53 gene mutation was noted at the first recurrence and progression to Grade II ganglioglioma and in the subsequent progression, to glioblastoma. Hence they inferred that the p53 mutation was a progression associated mutation and that the molecular pathways of gangliogliomas progressing to become glioblastoma is similar to that of diffuse astrocytomas progressing to become glioblastoma.14 In our study too, p53 positivity was noted in the astrocytic component of Grade II Gangliogliomas (astrocytic component of case 2 and 3) as well as in Grade III ganglioglioma, with values markedly higher in the Grade III ganglioglioma. The important differential diagnosis is dysembryoplastic neuroepithelial tumors (DNT). The distinguishing features are (1) DNT are usually intracortical, (2) these exhibit multinodularity, (3) foci of cortical Dysplasia are seen in adjoining cortex (4) there is high degree of cellular polymorphism, and (5) specific glioneuronal element is seen in the simple and complex forms.15 In our study, we have diagnosed 5 cases of Gangliogliomas in our department over a period of 5 years and have discussed in detail the pathological and Immuno-histochemical features of these tumors. In addition we have discussed the clinical presentation and radiological features of these tumours. REFERENCES
Copyright 2004 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn04008f6.jpg] [cn04008f4.jpg] [cn04008t2.jpg] [cn04008f1.jpg] [cn04008f8.gif] [cn04008f5.jpg] [cn04008f2.jpg] [cn04008t1.jpg] [cn04008f3.jpg] [cn04008t3.jpg] [cn04008f7.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}