 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
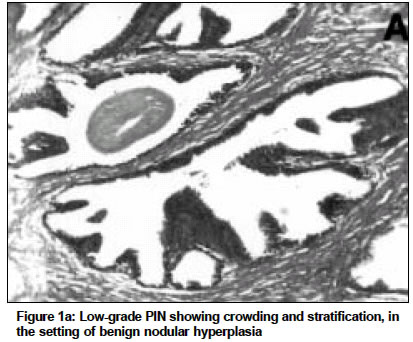
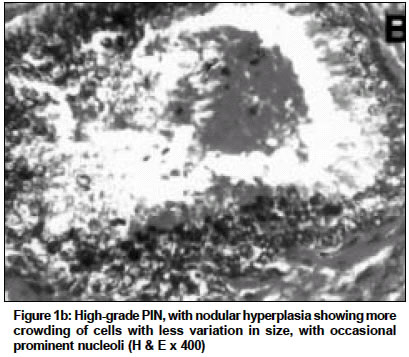
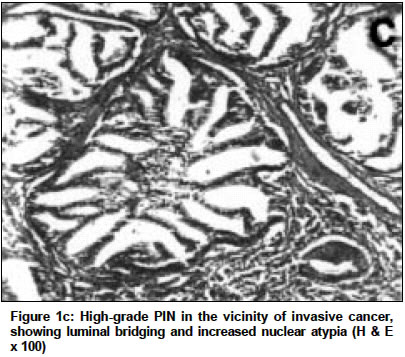
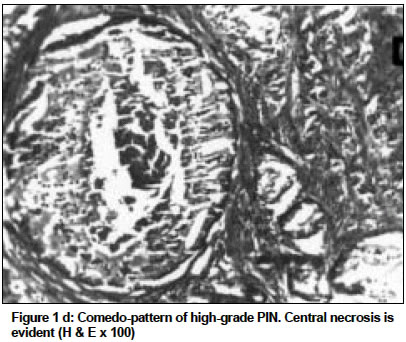
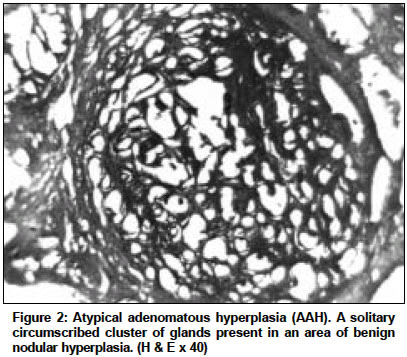
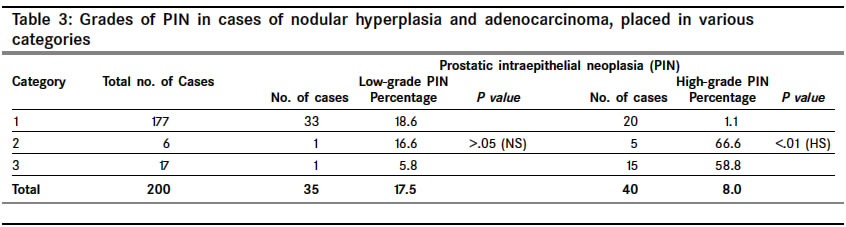
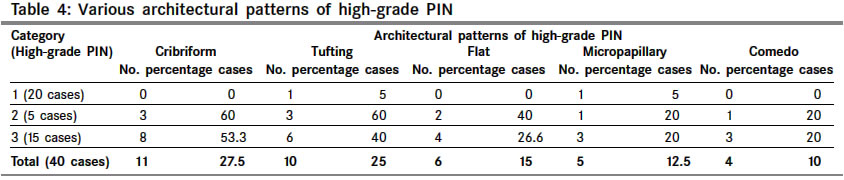
Indian Journal of Cancer, Vol. 41, No. 2, Apr-Jun, 2004, pp. 60-65 Original Article Premalignant lesions of prostate and their association with nodular hyperplasia and carcinoma prostate Rekhi Bharat, Jaswal TS, Arora B Institute of Pathology-ICMR, Safdarjung Hospital, New Delhi - 110029 Code Number: cn04011 ABSTRACT BACKGROUND: A relatively new development in the arena of prostatic histopathological study is the premalignant proliferative changes in the glandular epithelium, possibly relating to carcinoma. Two major categories have come up, namely prostatic intraepithelial neoplasia (PIN) and atypical adenomatous hyperplasia (AAH). AIMS: The aims of present study were to identify foci of the two putative premalignant conditions viz. PIN and AAH in ducto-acinar lining epithelia of 200 prostatectomy specimens and their association with nodular hyperplasia and adenocarcinoma prostate. MATERIAL AND METHODS: Micro sections from 200 prostatectomy specimens, received in the Department of Pathology, PGIMS, Rohtak, were extensively studied for the presence and association of premalignant conditions. Significant values were obtained by employing Chi-square (x2) test, with P value <0.05 as significant. RESULTS: Out of 177 cases of nodular hyperplasia, 53 (29.9%) showed PIN and 38 (20.3%) showed presence of AAH. All 6 cases (100%) of pure carcinoma revealed foci of PIN. Out of the remaining 23 cases of carcinoma with nodular hyperplasia, foci of PIN were observed in 16 cases (94.1%) and AAH in 2 cases (11.7%). High-grade PIN was observed in 20 cases (86.9%) of the total 23 cases of carcinoma, with/without nodular hyperplasia and 20 cases (11.2%) of nodular hyperplasia. Low-grade PIN was observed in 33 cases (18.6%) of nodular hyperplasia and in only 1 case (5.8%) of carcinoma prostate with nodular hyperplasia. CONCLUSION: PIN, especially high-grade type was the most commonly observed premalignant lesion, in cases of adenocarcinoma, thereby suggesting it to be the likely precursor of carcinoma prostate. AAH showed a weaker association with carcinoma. Keywords: Prostate, Prostatic intraepithelial neoplasia, Atypical adenomatous hyperplasia, Adenocarcinoma prostate. INTRODUCTION A relatively new development in the prostatic histopathology is the identification of premalignant conditions that can help in early diagnosis of prostate cancer. The concept of tumor development through a multistep via premalignant lesions has been well documented in a number of organs including uterine cervix, endometrium, gastrointestinal tract, and respiratory epithelium.[1] In case of prostate it is recent. Orteil[2] (1926) gave the first description of premalignant changes in prostate. Since then, a number of reports have appeared in literature describing these lesions with a wide range of synonyms. The term prostatic intraepithelial neoplasia (PIN) endorsed in 1989, is defined as a cytologic alteration in architecturally normal glands.[3] It comprises an intraluminal proliferation of the secretory epithelium revealing a spectrum of atypical cytological changes ranging from minimal changes to those that are indistinguishable from carcinoma.[4] Three grades of PIN were identified, according to criteria of McNeal and Bostwick.[5] However, now, PIN is divided into two grades (low-grade and high-grade) to replace the previous three-grade system. PIN 1 is considered as low-grade; PIN 2 and 3 as high-grade[3] [Figure - 1 a, b, c, d] The other putative premalignant prostatic condition, described first by McNeal,[6] is atypical adenomatous hyperplasia (AAH). It represents an architectural alteration in cytologically unremarkable glands[7] [Figure - 2]. PIN; especially high-grade assumes importance as the most likely precursor of carcinoma prostate because of its greater association with the latter. AAH is the other putative premalignant lesion and its more common association with nodular hyperplasia than adenocarcinoma makes it a possible premalignant lesion to transition zone adenocarcinoma. This study was undertaken to identify the association of premalignant lesions in prostatectomy specimens and their role as a precursor of carcinoma prostate. MATERIAL AND METHODS A total of two hundred prostatectomy specimens received in the Department of Pathology, PGIMS, Rohtak, were taken up for present study. Conventional haematoxylin and eosin (H and E) stained micro sections were examined and wherever necessary, special stains like Periodic Acid Schiff, Reticulin etc. were employed. The cases were extensively studied for the presence and association of premalignant conditions with nodular hyperplasia and carcinoma prostate. They were placed into either of the following categories: Category 1: Nodular hyperplasia and associated premalignant condition Gleason[8] grading system was used for carcinoma prostate. Set criteria were used for the diagnosis of the two premalignant conditions i.e. prostatic intraepithelial neoplasia (PIN) and atypical adenomatous hyperplasia (AAH). Grading criteria for PIN were those laid down by the consensus at a 1989 International Conference i.e. low-grade and high-grade PIN.[3] The presence of AAH /adenosis was defined using criteria of Epstein.[9] Simple statistical methods such as chi-square (x2) were used to determine significance between various observed parameters. A P-value of <0.05 was accepted as significant. RESULTS Out of the 200 cases, 177 cases (88.5%) were of nodular hyperplasia (category 1); 6 cases (3%) of adenocarcinoma prostate (category 2) and remaining 17 cases (8.5%) had both nodular hyperplasia and adenocarcinoma (category 3). Gleason[8] grading system was used in all 23 cases of carcinoma. All cases were thoroughly examined for presence of foci of premalignant conditions. Out of these 200 cases, a total of 101 cases (50.5%) (category 1 i.e. 78 cases and category 2 and 3 i.e. 23 cases) showed the presence of foci of PIN and/or AAH. All 23 cases of adenocarcinoma prostate revealed presence of premalignant lesions. [Table - 1]. These results show a strong association of premalignant lesions with adenocarcinoma prostate. The association was also found to be significant in cases of nodular hyperplasia (44.0%). Statistically, the association of premalignant lesions with cases of adenocarcinoma prostate was found to be highly significant (P < 0.01). In category 1, 53 cases (29.9%) showed presence of foci of PIN and 36 cases (20.3%) showed presence of foci of AAH, whereas category 2 revealed PIN in all six cases (100%). In category 3, foci of PIN were observed in 16 cases (94.1%) and AAH was observed in 2 cases (11.7%) [Table - 2]. Thus, PIN was found to be more closely associated with carcinoma whereas AAH was observed more in cases of nodular hyperplasia. A significantly higher percentage of PIN was found to be associated with carcinoma, whereas AAH was observed more in cases of nodular hyperplasia Statistically, the association of PIN with carcinoma was found to be highly significant (P < 0.01). Out of 53 cases of PIN in category 1, 33 cases (18.6%) showed presence of low-grade PIN, whereas high-grade PIN was observed in 20 cases (11.2%). In category 2, out of 6 cases of PIN, only 1 case (16.6%) revealed low-grade PIN, whereas 5 cases (83.3%) had foci of high-grade PIN. In category 3, out of 17 cases of PIN, 15 cases (88.2%) revealed high-grade and only 1 case (5.8%) showed presence of low-grade PIN [Table - 3]. Thus, high-grade PIN was more commonly associated with carcinoma, whereas low-grade PIN with nodular hyperplasia prostate. High-grade PIN revealed five morphological patterns viz., cribriform, tufting, flat, micropapillary and comedo, all with nucleomegaly and prominent nucleoli. These patterns merged with each other from gland to gland, although fields with only single pattern were occasionally observed. Cribriform was the commonest pattern observed in 3 cases (60%) of category 2 and 8 cases (53.3%) of category 3 [Table - 4]. Various other lesions were also identified with some normal anatomical structures that constituted as a differential diagnoses for the premalignant lesions. These included portions of seminal vesicle, along with foci of basal cell hyperplasia, cribriform hyperplasia, atrophy-associated hyperplasia, squamous metaplasia, transitional metaplasia and area(s) of infarction. Out of these, foci of basal cell hyperplasia were the most commonly observed other associated lesion and were observed in 46 cases (25.9%) of category I and 5 cases (29.4%) of category 3. Inflammation was the other commonly observed lesion in all the cases under study. Out of total 200 cases, 157 cases (78.5%) showed features of prostatitis, 3 cases (1.5%) of granulomatous prostatitis. Prostatits was observed in 151 cases (85.3%) of nodular hyperplasia and in 9 cases (38.6%) of adenocarcinoma, thereby reflecting its stronger association with the former. Out of 75 cases of PIN, prostatitis was observed in 51 cases (66.6%) [Table - 5]. DISCUSSION Early diagnosis of prostate cancer is an important issue among urologists and pathologists. A multidisciplinary approach using Digital rectal examination (DRE), transrectal ultrasound and prostate specific antigen assay has been adopted for early detection of prostate cancer. Despite these efforts, 33% of patients still present with advanced stage of the disease.[10] Identification of premalignant lesions assumes importance in this context. Lately, PIN and AAH have been recognized as putative premalignant lesions of prostate. However, the supportive evidence for PIN is much greater than AAH, with high-grade PIN being the most likely precursor, arising in the peripheral zone.[11] AAH has been presumed to be a precursor of well-differentiated transition zone carcinoma.[10] A wide variation in the incidence and prevalence of PIN in nodular hyperplasia has been reported in the world literature, ranging from 12.8% to 43 % in different studies.[5],[12],[13],[14] The association of PIN with adenocarcinoma has always been observed to be higher, as is evident from earlier studies, where it was observed to be 76% to 100%.[5],[11],[15],[16] Our findings revealed an intermediate frequency of PIN in BPH cases (29.9%), between the lowest and highest observed results. Low-grade PIN was the most commonly observed grade in cases of nodular hyperplasia, whereas cases of adenocarcinoma showed high-grade PIN as the most commonly observed grade (86.9%). Earlier investigators[17] have reported low-grade PIN in 14-81% cases of nodular hyperplasia and a higher grade of PIN in carcinomatous prostates, reflecting a greater possibility of high-grade PIN as a precursor lesion to carcinoma prostate. This is in keeping with the terminology of premalignant lesions in the light of multistep theory of carcinogenesis.[18] A significant association (88.2%) of high-grade PIN with cases of nodular hyperplasia and adenocarcinoma (category 3) in our study indicates the existence of "field" effect that the carcinoma casts on the adenomatous zone. Thus, the presence of high-grade PIN in the adenomatous zone in cases of nodular hyperplasia requires a follow-up. Various architectural patterns of high-grade PIN in cases of carcinoma (with or without nodular hyperplasia) in form of cribriform, tufting, flat, micropapillary and comedo forms have been reported by several authors, with variable frequencies.[15],[19],[20] We identified pure cribriform pattern as the commonest (55%). Several other associated lesions and normal anatomical structures entered as a differential diagnoses like portions of seminal vesicle; foci of basal cell hyperplasia, cribriform hyperplasia, squamous metaplasia etc. Bostwick and Srigley[21] have also given a detailed account of such lesions. They also stated that basal cell hyperplasia commonly merges with areas of nodular hyperplasia. However, according to Grizzle W,[22] basal cell hyperplasia could have a role as a precursor of adenocarcinoma on the basis of sequential changes. Thus, these views seem to be two opposite points on the horizon with gaps to be filled or at least suitably bridged and interconnected. Other studies also share the idea of considering basal cell hyperplasia as an important precursor lesion to prostatic carcinoma basaloid type.[23],[24] In the present study, identification of basal cell hyperplasia as the commonest other associated lesion in 25.5% cases implies that it could have a role as a precursor to adenocarcinoma as it can be explained on the basis of sequential changes of basal cell hyperplasia-low grade PIN-high-grade PIN-cancer. Srigley et al[11] observed foci of AAH in 19.6% cases of the BPH and a higher percentage (60%) in carcinoma cases, whereas Qian J et al[15] noted 31% association of AAH with prostate carcinoma. Our study revealed AAH in 20.6% cases of nodular hyperplasia and only 2.6% cases of adenocarcinoma. The lower percentage association of AAH with adenocarcinoma in our study might possibly have been due to small sample size of cases of carcinoma and perhaps small sample artifacts since the data reported in the literature is based upon autopsy studies and also whole mounted specimens. A significant association of prostatits, more with nodular hypeplasia than adenocarcinoma prostate suggests that the possibility of "field effect" caused by inflammation in the neighboring areas also exists, but warrants search for genuine carcinoma [Table - 5]. Thus, it is suggested that in cases of PIN, especially higher-grade, patients need close follow-up observations and investigations to rule out existence of carcinoma, especially in the peripheral zone. Davidson et al[25] found adenocarcinoma in 35% of subsequent biopsies for patients with previous diagnosis of PIN, compared with 13% in a control group without PIN. Therapeutically, a marked decrease in the prevalence and extent of high-grade PIN has been observed in patients with androgen deprivation therapy (ADT), as compared to untreated prostates.[16],[26] Thus, dysplastic prostatic epithelium is hormone dependent and ADT reduces proliferation and enhances apoptosis. Occurrence of AAH needs thorough search and follow up for presence of intermediate zone low-grade adenocarcinoma. Basal cell hyperplasia must be treated with respect because of its possible role as an initial lesion in the train of events progressing to full blown carcinoma through stages of PIN. Infact, there is need of identifying other types of precursor lesions from which adenocarcinoma develops ACKNOWLEDGEMENTS I am highly grateful to the Professor and Head, Department of Pathology, Pt.B.D. Sharma, Post Graduate Institute of Medical Sciences, Rohtak, for helping me carry out this work.REFERENCES
Copyright 2004 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn04011f2.jpg] [cn04011f1c.jpg] [cn04011f1b.jpg] [cn04011t1.jpg] [cn04011f1d.jpg] [cn04011f1a.jpg] [cn04011t2.jpg] [cn04011t5.jpg] [cn04011t3.jpg] [cn04011t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}