 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
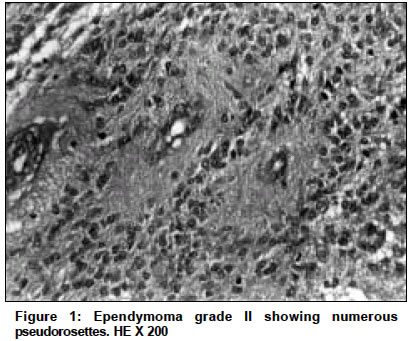
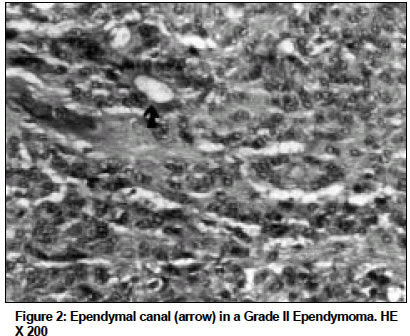
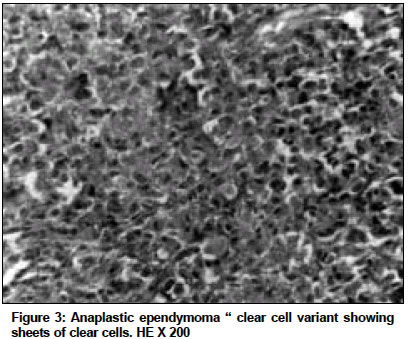
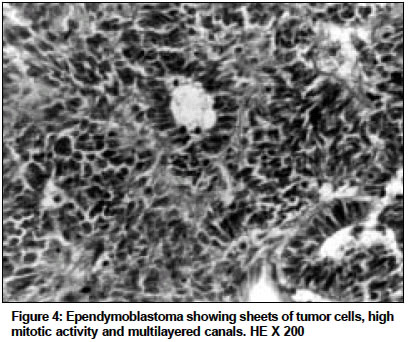
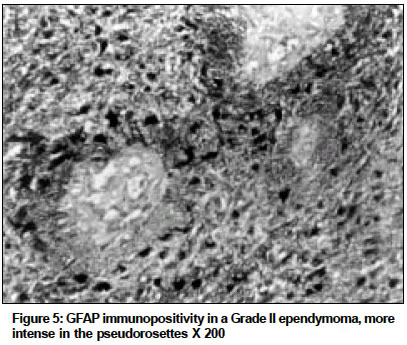
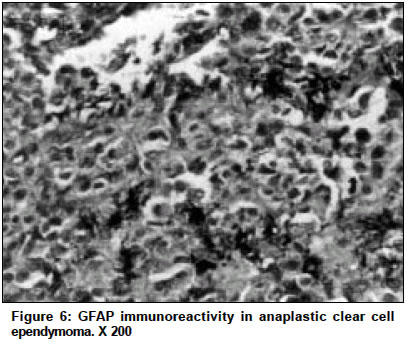
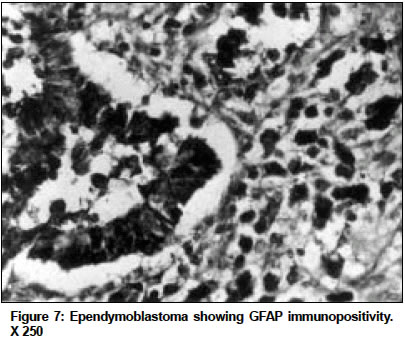
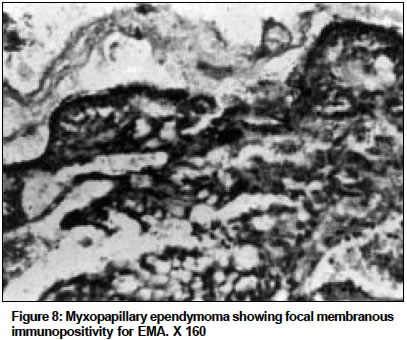
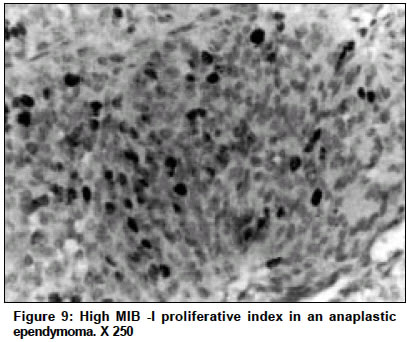
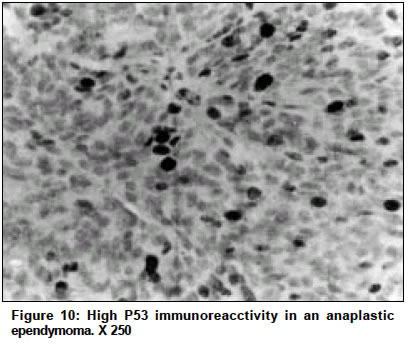
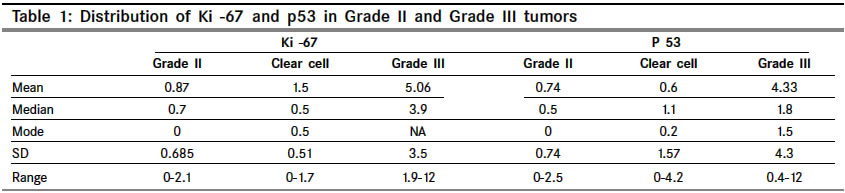
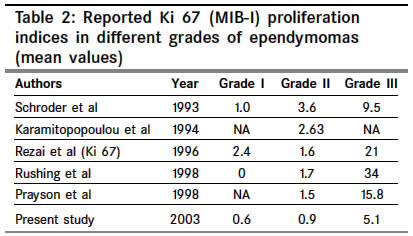
Indian Journal of Cancer, Vol. 41, No. 2, Apr-Jun, 2004, pp. 66-71 Original Article Histological spectrum of ependymomas and correlation of p53 and Ki- 67 expression with ependymoma grade and subtype Suri VaishaliS, Tatke Medha, Singh Daljit, Sharma Ajay Departments of Pathology, G. B. Pant Hospital, New Delhi - 110002 Code Number: cn04012 ABSTRACT BACKGROUND: Clinical and histological criteria for ependymoma prognosis are well recognized. Recently few studies have been done based on Immunohistochemistry for prognostication of these tumours. In this study we have correlated the histlogical spectrum with immmunoexpression of p53 and Ki67 in these tumors. AIMS: To know the incidence of ependymomas; study their morphological spectrum and to evaluate expression of P53 and Ki 67 in diffferent morphological subtypes. MATERIAL AND METHOD: A retrospective sudy was preformed on 70 ependymomas received in a period between 1994 and 2001. Entire tissue received was processed for routine paraffin embedded H&E stained sections. Immunocytochemistry was performed using antibodies to GFAP, EMA, Pancytokeratin and synaptophysin, to differentiate papillary ependymoma from choroid plexus papilloma; clear cell ependymoma from oligodendroglioma and central neurocytoma; ependymoblastoma from other embryonal tumours. p53 and Ki-67 immunohistochemistry was performed to correlate their expression with various tumour grades and subtypes. RESULTS: There were 3 cases (4.2%) of Grade I ependymoma (2 cases of myxopapillary ependymoma and 1 case of subependymoma); 57 cases (81.5%) of ependymoma grade II (43 of these were of classical variety, 11 of clear cell ependymoma, 2 of papillary and 1 case of cellular ependymoma). There were 9 cases (12.8%) of anaplastic ependymoma (one of these was a clear cell ependymoma and 1 case (1.5%) of ependymoblastoma CONCLUSION: p53 and Ki67 indices can be used in routine diagnostic laboratories to supplement the tumor grade on histology and more studies with follow up should be performed toanalyse the prognsis of different subtypes. The expression of Ki 67 and p53 was significantly higher in anaplastic ependymomas. 4 out of 11 cases of clear cell ependymomas showed higher Ki 67 indices as compared to classical grade II ependymomas, thus further highlighting the importance of differentiating the various subtypes. Keywords: Ependymoma, Immunohistochemistry, Ki- 67, p53. INTRODUCTION Ependymomas constitute approximately 3-5% of all intracranial malignancies and are the third most common brain tumours in children after pilocytic astrocytoma and medulloblastoma.[1],[2],[3],[4],[5] Most ependymomas in adults are intraspinal, but in children, these tumours develop preferentially in the posterior fossa where they arise from the fourth ventricle ependymal cells.[2],[6] The prognosis remains poor, regardless of introduction of radiotherapy and or chemotherapy in the treatment protocol. Age, surgical removal, tumour location and histology have been evaluated as important factors affecting survival,[7] however relevance of each of these variables and their possible combinations in limiting the prognosis are still unclear. More recently p53 and Ki -67 have been widely used as markers to predict outcome in various malignancies.[8],[9],[10] The p53 gene is a tumour suppressor gene located on the 17p13.1 and is the single most common target for genetic alterations in human cancer. Ki -67 is an established marker for proliferative index in cycling cells.[11] Its presence in large proportion of cells suggests an aggressive neoplasm. Investigation into role of these antigens in neuroectodermal tumors have concentrated primarily on astrocytic tumors.[2],[4] Recently some authors have advocated that Ki 67 and p53 immunolabelling are important prognostic markers in ependymomas.[12],[13],[14] In present study we have studied the morphological spectrum of ependymomas and correlated p53 and Ki67 expression with various tumor grades and subtypes. MATERIAL AND METHODS A retrospective study was conducted in Department of Pathology. G. B. Pant Hospital. New Delhi. There were 70 ependymornas out of 2679 CNS tumors received over a period of 8 years. These tumors were sent with a provisional diagnosis of choroid plexus papilloma, ependymoma, oligodendroglioma, astrocytoma, glioblastoma, meningioma, PNET, and medulloblastoma. Entire tissue received was processed for paraffin embedded sections. The diagnosis was made on H and E stained, 3-4 µm thick sections. Immunocytochemistry by the labelled Streptavidin Biotin technique using antibodies to GFAP, Synaptophysin, EMA and Pancytokeratin (all were prediluted, from DAKO Carpinteria. CA) was performed. Immunocytochemistry with antibodies to p53 (prediluted, DAKO DO-7) and Ki-67 (prediluted, Novocostra. Newcastle upon Tyne) was performed to evaluate their expression in the tumour, grades and histological subtypes. Sections from Grade III Astrocytoma (for GFAP, p53 and Ki 67), normal oesophageal biopsy (for EMA), Normal cortex and white matter (for Synaptophysin ) were used as positive controls. All the slides were seen by two observers. Interobserver variation was minimal. For calculating the indices, the observers were blinded to the grade of the tumor. These were calculated by counting positive nuclei of cells in 10 separate fields within adjacent fields of the area with the highest density of labeled cells at 400x magnification. Atleast 1000 neoplastic cells were analysed and ratio of total number of positive nuclei and total number of tumor cells was taken as labeling index. Tumor vascular component and hemorrhagic areas were excluded. The difference in expression of p53 and Ki 67 various tumor grades and subtypes was evaluated using student′s T Test Histological criteria used for typing and grading of tumors were according to recent WHO classification of tumors [13]. Myxopapillarv ependymomas (grade I) are characterized by cuboidal to elongated tumor cells around vascularized stromal cores in a mucoid matrix. In grade II ependymomas there are perivascular pseudorosettes, ependymal canals, rare or no mitosis. Grade III (anaplastic) ependymomas show increased cellularity, brisk mitotic activity, vascular proliferation, endothelial hyperplasia, pseudopallisading necrosis, perivascular rosettes and ependymal canals. In epndymoblastoma, high cellularity, numerous multilayerd canals and high mitotic activity is seen. RESULTS A total of 70 ependymomas were diagnosed out of 2679 CNS tumors received over a period of 8 years (Jan 1994- Jan 2002), accounting for an incidence of 2.6%. There were 58 cases of intracranial ependymomas (incidence =2.16%). These were located in cerebral hemisphere (16), lateral ventricle (3). Pineal (1), 4th ventricle (37) and CP angle (1). There were 12 cases of spinal ependymomas (incidence = 0.4%). 7 of these were intramedullary and 6 were intradural extramedullary. A majority of these (42%) were located in the dorsal spine followed by cervical (33%), filum (17% ) and lumbar regions (8%). The age group of patients varied from 1-61 years. There were 50 males and 20 females. The majority of spinal cases were in age group > 30 years (mean age = 40 years) and amongst the intracranial cases, majority were below 40 (mean age = 23 years). There were 3 cases (4.2%) of Grade I ependymoma (2 cases of mvxopapillarv ependymoma and 1 case of subependymoma); 57 cases (81.5%) of ependymoma grade II (43 of these were of classical variety [Figure - 1] and [Figure - 2], 11 of clear cell ependymoma, 2 of papillary and 1 case of cellular ependymoma). There were 9 cases (12.8%) of anaplastic ependymoma (one of these was a clear cell ependymoma [Figure - 3] and 1 case (1.5%) of ependymoblastoma [Figure - 4]. Distribution of GFAP and EMA was variable amongst various tumor grades. GFAP immunopositivity was mainly seen in the ependymal cells and the cell processes forming the perivascular pseudorosettes [Figure - 5]. In some cases, cells forming tubules, and more solid groups showed positive cytoplasmic staining [Figure - 6] and [Figure - 7]. Diffuse GFAP immunopositivity was maximum in low grade (Grade II) tumors (85.9% cases) as compared to grade III tumors (62.5% cases) The tumor cells showed membranous positivity for EMA, which was either focal or was distributed uniformly throughout the tumour [Figure - 8]. Diffuse expression of EMA was slightly higher in grade III tumors as compared to Grade II tumors (55.5% vs 47.4 %). The mean Ki-67 and p53 proliferative indices [Figure - 9] and [Figure - 10], were significantly higher in grade III tumors (5.1 and 4.3%) as compared to grade I (0.6 and 0.1%) and grade II tumors ( 0.9 and 0.7%). The difference in expression for both Ki67 and p 53 was highly significant between grade II and grade III tumors (P value < 0.0001). There was only one case of ependymoblastoma in which Ki-67 index was 13% and p53 index was 18%. The range for both these indices was maximum in grade III tumors. It varied from 1.9 - 12% for Ki-67 and 0.4 - 12% for p53. 4 out of 11 cases of clear cell ependymomas showed higher ki 67 labeling indices as compared to classical grade II ependymoma, but the difference was not statistically significant (mean Ki67 and p53 indices in clear cell ependymomas was 1.5 and 0.6 respectively). The mean, median, mode and range of p53 and Ki67 in various tumor grades have been highlighted in [Table - 1]. There were only 2 cases of papillary ependymomas and the Ki -67 and p53 indices were not different from classical grade II ependymomas. However more cases are required to comment upon the usefulness of these markers for determining the prognosis in these subtypes of grade II ependymomas. DISCUSSION The correlation of histopathological parameters like mitosis, anaplasia, necrosis and endothelial hyperplasia with outcome in ependymomas has been notoriously erratic. Although tumors are classified as being of either low grade or anaplastic/malignant based on presence of a constellation of worrisome histological features, the correlation between assigned histological grade and clinical outcome is not always good.[15] Analysis of individual histological features in survival stuies identifies virtually none with convincing prognostic value.[4],[16],[17],[18] The prognostic significance of other factors like patient′s age, tumor location, volume of resection, protocols of adjuvant therapy have been intensively examined but numerous studies have yielded conflicting results,[19] The present study was conducted with the objectives of knowing the incidence of ependymomas and the various morphological types; to evaluate the expression of p53 and Ki- 67 in different morphological types. Expression of p53 and Ki 67 was correlated with the grade of tumor. The mean Ki -67 and p53 indices were significantly higher in grade III tumors as compared to grade I and II tumors. The difference in expression of Ki67 and p53 was highly significant between grade II and grade III tumors (P value < 0.0001). Many authors have studied the expression of Ki 67 and Ki si in various Grades of in various Grades of ependymomas and in recurrent tumors.[12],[13],[14],[15],[19],[20],[21] These authors have indicated that the Ki- 6 7 labelling index is confirmed as a very important prognostic marker for ependymaomas. [Table - 2] shows a comparison of results in Ki 67 (MIB I) expression in various grades of ependymomas from different studies done since 1993, including the present study[12],[13],[14],[15],[22],[23],[24] However the MIB - I indices shows variable results in different studies. This is probably due to lack of uniformity used in specimen storage, various biopsy samples, difference in intensity of nuclear stains, techniques used and subjectivity in evaluation. Although p53 gene alterations have been frequently documented in malignant gliomas, loss or mutations of wild type p53 have only a limited role in tumorogenesis of ependymomas according to various authors.[25],[26] However recently some authors have documented a correlation between p53 expression and tumor grade in ependymomas.[12],[13] Verstegen et al and Korshunov et al in their studies have claimed aberrant p53 expression to be one of the strongest predictors of a worse survival.[14],[19] In our study, 4 out of 11 cases of clear cell ependymomas showed slightly higher Ki 67 indices as compared to classical grade II ependymomas, but the difference was not statistically significant. Suzuki et al. in 2001 in their study on 29 patients of ependymoma advocated that the clinical course was worst in clear cell ependymoma which had significantly higher expression of MIB -I and p53 than the other subtypes.[13] Our study highlights that p53 and Ki 67 indices when performed in routine diagnostic cases can supplement the histological diagnosis and at the same time these values could predict the relative difference in prognosis of various subtypes. But for this more studies have to be done with long term follow up of these patient. Unfortunately we could not do the follow up as post operative radio and chemotherapy is not available in our hospital To summarize, in our study the incidence of ependymomas was 2.6%, the commonest type being classical grade II ependymomas (81.5%). Both Ki-67 and p53 expression correlated with tumor grade and the expression of both Ki -67 and p53 was significantly high in anaplastic ependymomas. More studies of this type along with long term follow up are required to establish definite and uniform criteria and cut off values to inculcate these antibodies as markers of prognosis and survival prediction in ependymomas. REFERENCES
Copyright 2004 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn04012t1.jpg] [cn04012f9.jpg] [cn04012f3.jpg] [cn04012f8.jpg] [cn04012f5.jpg] [cn04012f6.jpg] [cn04012f4.jpg] [cn04012f2.jpg] [cn04012f7.jpg] [cn04012t2.jpg] [cn04012f1.jpg] [cn04012f10.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}