 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
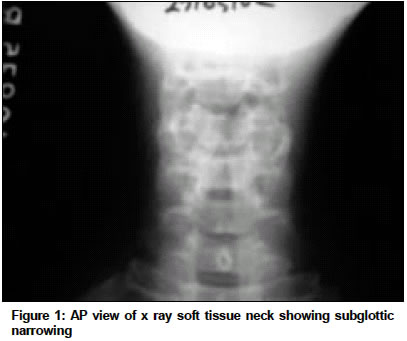
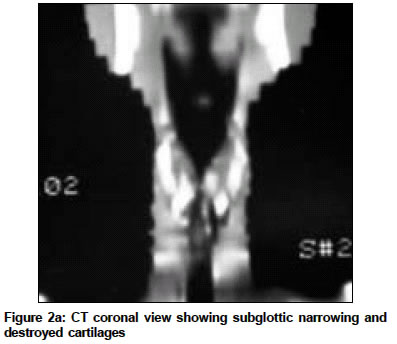
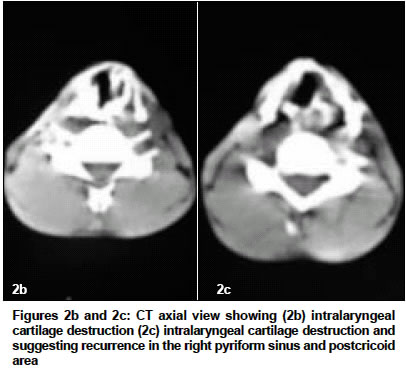
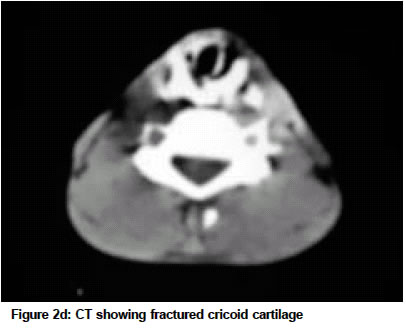
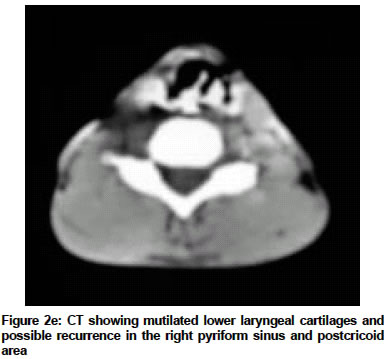
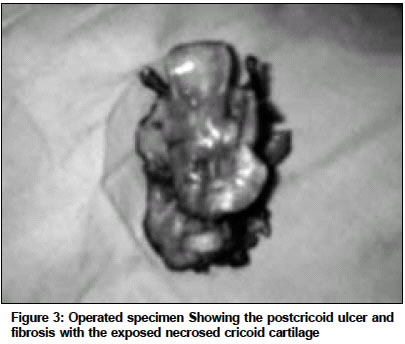
Indian Journal of Cancer, Vol. 41, No. 2, Apr-Jun, 2004, pp. 81-84 Case Report Late post radiation laryngeal chondronecrosis with pharyngooesophageal fibrosis Varghese BipinT, Paul S, Elizabeth MI, Somanathan T, Elizabeth KA Department of Surgical Oncology, Regional Cancer Centre, Trivandrum - 695011 Code Number: cn04014 ABSTRACT Chondroradionecrosis of larynx is a well recognized complication of radiation therapy, which usually occur with in the 1st year. Review of literature shows very few accounts of late radiation induced clinical chondroradionecrosis of the larynx. This condition can mimic a local recurrence and severe and life threatening involvement will require aggressive surgical management as reported in the present case. Keywords: Chondroradionecrosis, Fibrosis, Laryngopharyngectomy INTRODUCTION An unusual case of symptomatic late chondroradionecrosis of larynx with fibrosis and stricture of the pharyngooesophageal segment is reported. Medline search indicates that the present case report is the severest of its nature, necessitating aggressive surgical extirpation and reconstruction on an emergency basis. The current literature is reviewed and the indications for surgical intervention in such situations discussed.CASE REPORT A 38-year-old man radically irradiated for carcinoma of the Right Vocal cord (T1NoMo) in 1994 presented to our department with moderate stridor on 25/9/02. The stridor was slowly progressive with associated cough and he was already on antibiotics and steroids prescribed from elsewhere. He also had undergone direct laryngoscopy (DLS) thrice from the same center during the course of his current illness, all of which were negative for tumour recurrence. Indirect laryngoscopy (IDL) revealed fixity of. right hemilarynx and a subglottic fullness on the right side, suggestive of submucosal recurrence. Anteroposterior (AP) view of x ray soft tissue neck revealed subglottic narrowing [Figure - 1] He could not co-operate for a direct laryngoscopy under local anaesthesia, due to stridor. Since he did not consent for a tracheostomy further attempts were not made and was given a further course of steroids for his stridor. Although he was asked to come after a week for direct laryngoscopy, he reported to us after a gap of 2 weeks with aggravation of stridor and choking spells with odynophagia and severe dysphagia to solids and semisolids. He also had severe aspiration on taking liquids. On examination there was splaying of laryngeal cartilages, cartilage tenderness and laryngeal crepitus was felt. He was admitted with a course of further antibiotics, steroids and intravenous fluids. CT scan of the larynx and hypopharynx suggested recurrence in the larynx and hypopharynx with additional features of destruction of laryngeal cartilages [Figure - 2a], Figure - 2b-c, Figure - 2d, [Figure - 2e]. A direct layngoscopy was then carried out after a tracheostomy which confirmed the clinical and radiological findings. The entire larynx and hypopharynx was oedematous (Rt > Lt) and the post cricoid area showed an ulcer on the right side. The subglottis was narrowed to 1/3rd by a mucosal bulge on the right side. Postcricoid area was narrowed and a no14 nasogastric tube passed with difficulty However the biopsy taken from suspicious areas (oedematous and ulcerated mucosa) in the endolarynx and hypopharnyx were negative. A repeat DLS and biopsy done after 1 week of hospital stay was again negative. With a strong suspicion of chondronecrosis of the laryngeal skeleton a surgical salvage was planned for the life threatening radiation sequelae after a detailed informed consent. The patient and relatives were informed that the surgery was being done to remove the larynx which has been severely mutilated by a late radiation sequelae and his post operative Histopathology report (HPR) also may not show viable tumour cells. Probable poor outcome in the event of the operated specimen being positive for malignancy was also duly explained. The salvage surgery was undertaken on 30/10/02. Peroperatively the disease process was found to extend significantly to the postcricoid area and adjacent cervical oesophagus. The entire post cricoid mucosa was thickened and a 1.5 x 1.5 cm ulcer with exposed necrosed cricoid cartilage was seen [Figure - 3]. The postcricoid region and adjacent cervical oesophagus was partly stenotic thickened and friable. Thyroid isthmus and both lobes were found to be adherent to trachea and the tracheoesophageal groove (suggestive of macroscopic tumour invasion) the entire larynx with the unhealthy pharyngoesophageal segment and adjacent overlying thyroid was excised widely [Figure - 3] The pharyngoesophageal continuity was then restored with a tubed Pectoralis Major Myocutaneous Flap (P.M.M.C) flap. The postoperative period was uneventful. The laryngopharyngectomy specimen on microscopic examination showed ulcerated stratified squamous epithelium with no evidence of any recurrent neoplasm. The laryngeal cartilage showed necrosis and fragmentation with inflammatory cell infiltration around it. Some of the lobules of cartilage showed sequestrated bone surrounded by inflammatory cell infiltration proliferated fibroblasts and capillaries. DISCUSSION Chondroradionecrosis of larynx and fibrosis with stricture of the pharyngooesophageal segment is a well recognized complication of radiation therapy. However they usually occur with in the 1st year. Review of literature showed very few accounts of late radiation sequelae of larynx and hypopharynx.[1],[2],[3],[4],[5],[6] Keene et al in their study on 265 laryngeal specimens received after eradication of primary squamous cell carcinoma noted histologic chondronecrosis in 26% of them although only 3% of them were clinically diagnosed to have laryngeal chondronecrosis. Factors predisposing to the onset of laryngeal chondroradionecrosis are 1) dose and technique of RT 2) portals of RT 3) Frequency of RT 4) stage of tumour 5) Trauma before or after RT 6) Infection.[1],[2],[3],[4],[5],[6] Unlike osteonecrosis, chondronecrosis is possible only when the cartilage is exposed. Management of chondronecrosis of larynx is essentially conservative except in the most severe and symptomatic forms.[5] Conservative surgery in the form of debridement and replacement of lost tissue can be done if the laryngeal framework involvement is very limited.[7] Reconstruction of the sacrificed diseased tissues can be achieved with a muscle,[7] myocutaneous (for eg PMMC flap) or a free flap. We believe that the present case is the most severe form of symptomatic late radiation sequelae affecting both larynx and hypopharynx, ever reported in literature. The clinical and radiological presentation clearly mimicked a local recurrence and the final exclusion of coexistent recurrence was made only after a detailed histopathological study of the specimen by serial sectioning which showed presence of chondronecrosis and fibrosis. Repeated intralaryngeal manipulation in the form of direct laryngoscopies and punch biopsies for suspected recurrence is probably the most significant factor that might have lead to the present complication. Decision for surgical interference was guided by the life threatening symptoms including airway obstruction, aspiration, severe dysphagia and odynophagia. The above case is presented to highlight an unusual, life threatening, late post radiation sequelae, which necessitated a total laryngopharyngectomy. The clinical and radiological picture simulated a transglottic recurrence of the tumour though repeated biopsies were negative. It is well known that even in presence of clinically frank residual/recurrent disease at times it is difficult to demonstrate histologically, viable malignant cells in the punch biopsy specimen taken endoscopically, because of the effect of radiotherapy at the periphery of the disease. Although CT scans and MRI accurately delineates malignant tumor and its extend at presentation, after radiotherapy it often fails to distinguish residual / recurrent disease from radiation sequelae.[8] This paper hence emphasizes the need for formulating guidelines for salvage surgery under such circumstances. The current guidelines followed at our department for salvage laryngectomy after 3 consecutive negative biopsies in clinical residual/recurrent carcinoma of larynx/hypopharynx are
CONCLUSION Late chondronecrosis of the laryngeal framework and fibrosis with stricture formation of the hypopharynx is a very rare complication of radiotherapy, which can clearly mimic a local recurrence. High index of suspicion and repeated negative biopsies points towards the diagnosis. Severe and life threatening involvement will require aggressive surgical management, which can even result in a total laryngopharyngectomy. Final conclusion about absence of a coexistent recurrence can be arrived at only after a detailed histological study of several cross-sections of the operated specimen.REFERENCES
Copyright 2004 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn04014f3.jpg] [cn04014f2e.jpg] [cn04014f1.jpg] [cn04014f2b-c.jpg] [cn04014f2a.jpg] [cn04014f2d.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}