 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
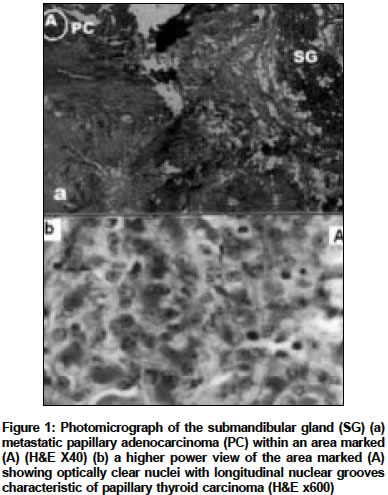
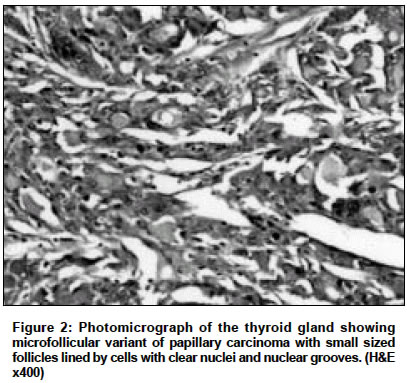
Indian Journal of Cancer, Vol. 41, No. 2, Apr-Jun, 2004, pp. 89-91 Case Report Isolated submandibular gland metastasis from an occult papillary thyroid cancer Sarda AK, Pandey D, Bhalla SA, Goyal A Department of Surgery, Maulana Azad Medical College & Lok Nayak Hospital, New Delhi - 110002 Code Number: cn04016 ABSTRACT A case of an isolated submandibular gland metastasis from a clinically occult papillary thyroid carcinoma is described in a 46-year old lady. Initial surgery was done based on the fine needle aspiration cytology (FNAC) report of adenocarcinoma of the submandibular gland. Histopathologic examination of the specimen suggested a metastatic papillary carcinoma. Occult papillary carcinoma in the thyroid was found by multiple blind FNACs. Subsequently to near-total thyroidectomy, no other site of metastasis was found on radio-iodine scanning. Keywords: Thyroid gland, papillary carcinoma, salivary gland, submandibular gland, metastasis INTRODUCTION The involvement of the salivary glands by metastatic tumors is rare. The Armed Forces Institute of Pathology estimates 10% of all malignant salivary gland tumors are metastatic.[1] Such rare metastases to salivary glands definitely involve the parotid gland much more than the submandibular glands, partly because of the differences in the number and anatomic relationships of the lymph nodes and their drainage.[2] While metastases to the parotid gland as the first clinical evidence of primary occult thyroid carcinoma are well described,[3] isolated metastases to the submandibular gland from thyroid papillary carcinoma have not been reported yet. We present a case of isolated metastasis to the submandibular gland as the first clinical evidence of primary occult thyroid carcinoma.CASE REPORT A 46-year old, two-year post-menopausal lady presented with a progressively increasing swelling in the left submandibular region of two years duration. There was neither history of pain nor increase in size of the swelling during meals The skin overlying the swelling had ulcerated two months prior to her presentation. Her medical history was unremarkable. She did not suffer from bone pains, cough or haemoptysis; no changes in urinary or bowel habits or uterine spotting were noted. She was not a known diabetic or hypertensive nor was there any family history of tuberculosis. On examination no pallor, cyanosis, clubbing or generalized lymphadenopathy were present. The thyroid gland was not enlarged and had a smooth surface. Both the breasts were normal. In the neck region, there was a mass, 7 cm x 6 cm in size, arising from the submandibular gland and protruding from the undersurface of the mandible till the level of the hyoid bone. The swelling was nodular, non tender and not fixed to the mandible, but the overlying skin was focally ulcerated The draining cervical lymph nodes were not enlarged. The hematological and biochemical investigations were within normal limits. X-rays of the chest and neck were also normal. Fine needle aspiration cytology (FNAC) of the swelling suggested an adenocarcinoma. The patient underwent excision of the submandibular gland with the left-sided radical neck dissection in view of the large size of the tumor and the presence of skin involvement. Histopathologic examination revealed a metastatic papillary carcinoma in the submandibular salivary gland, the lymph nodes being free of malignant deposits. [Figure - 1] Postoperatively, a thorough examination failed to reveal any abnormality in the thyroid, breasts, lungs, or abdomen. Mammography of both breasts and ultrasound of the abdomen were essentially normal. Radionuclide thyroid scan did not show any "cold" areas. Blind FNACs of the thyroid gland revealed papillary thyroid carcinoma and the patient subsequently underwent near-total thyroidectomy. On histopathologic examination, there were two 7 mm size foci of microfollicular variant of papillary thyroid carcinoma without extracapsular extension. [Figure - 2] Six weeks later, radio-ablation of the left thyroid was performed. At follow-up, no residual tumor in the neck nor distant metastases were found. The patient is well without recurrent or metastatic disease after a five year follow up. DISCUSSION Rarely, patients with clinical occult thyroid papillary carcinoma may present with a metastatic cervical lymphadenopathy;[4] however, distant metastases from an occult papillary thyroid carcinoma are extremely rare. There are even reports of ectopic thyroid tissue in the submandibular gland;[5] however, to our knowledge, there has been no previous report of an isolated metastasis from an occult papillary thyroid carcinoma to the submandibular gland. The exceptional rarity of this occurrence can be gauged from the fact that only 1% to 4% of all head and neck tumors are malignant neoplasms of the major salivary glands.[1] Metastatic tumours account for approximately 3% of malignant salivary gland neoplasms and only 10% to 20% of such metastatic tumours occur in the submandibular glands.[1] Among all the salivary gland tumors, 85% occurred in the parotid gland of which 18% were malignant, 7% were in the submandibular gland of which 37% were malignant, and 8% in the major sublingual and the minor salivary glands of which 47% were malignant.[6] However, tumors metastatic to the salivary glands are rare and more often located in the parotid gland (80-90%) In the parotid gland, metastatic tumors constitute 10% of all the malignancies and 40% are melanoma, 40% are squamous cell carcinomas, the remaining being from primary sites in the head and neck region, predominantly the scalp and ear, and rarely, thyroid and tonsils. Metastases to the submandibular gland are even rarer (10% to 20%).[1] In fact, till 2001, metastatic spread to the submandibular gland had been reported on 11 occasions,[8] being usually infraclavicular in origin, coming from the breast, lungs or kidneys[8] and even the urinary bladder, colon and liver.[9] Thus, whereas metastases to the parotid gland are primarily from the head and neck region and spread is mainly by lymphatic route, the majority of metastases to the submandibular gland are from a distant source and spread is by a haematogenous route.[1] Possibly, this difference lies in the scarcity or total absence of lymphoid tissue inside the submandibular gland, while the parotid gland may contain more than a lymph node tissue within its capsule.[10] While the extensive lymphatics surrounding the parotid gland make it susceptible to metastases from head and neck tumors, paucity of lymphatic tissue surrounding the submandibular gland protects it from such spread.[8] In conclusion, in 84% of cases, a palpable lesion in the submandibular gland is a primitive salivary gland tumor;[6] metastatic tumors are rare. This report wants to emphasize that a metastasis from an occult neoplasm must be considered whenever an unusual carcinoma in seen in a salivary gland, especially the submandibular gland. REFERENCES
Copyright 2004 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn04016f2.jpg] [cn04016f1.jpg] |
| |||||||||

{kind=link}
{kind=link}