 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
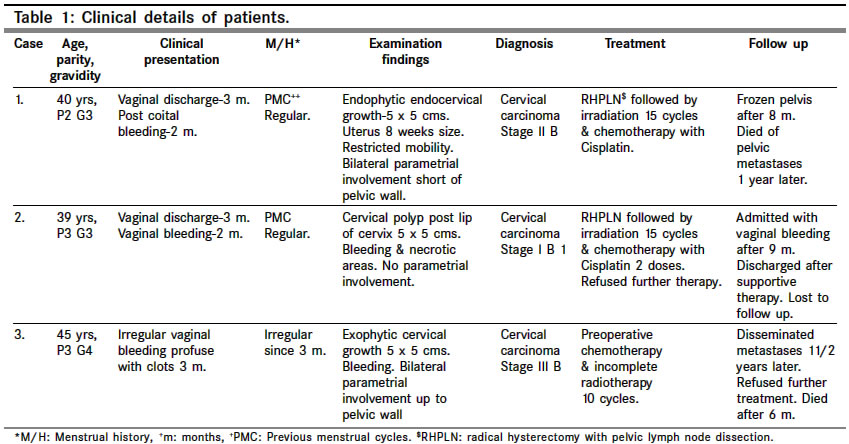
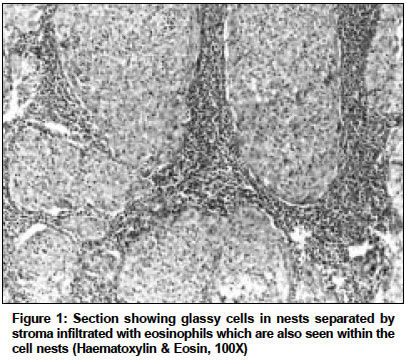
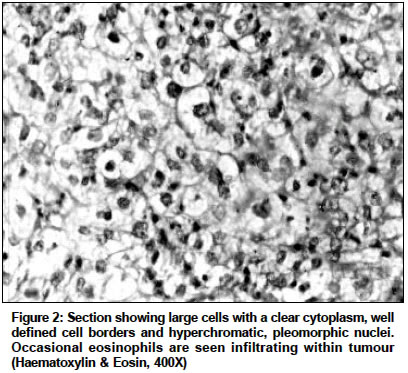
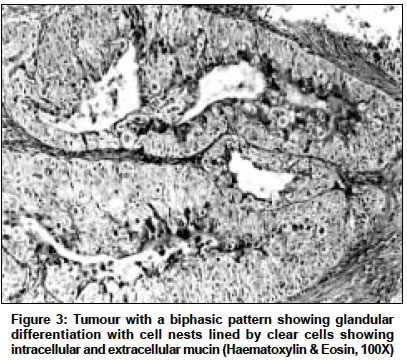
Indian Journal of Cancer, Vol. 41, No. 2, Apr-Jun, 2004, pp. 92-95 Case Report Glassy cell carcinoma of the uterine cervix a rare histology. Report of three cases with a review of the literature Deshpande ArchanaH, Kotwal MN, Bobhate SK Department of Pathology, Government Medical College, Nagpur Code Number: cn04017 ABSTRACT Glassy cell carcinoma is a poorly differentiated variant of adenosquamous carcinoma of the cervix associated with an aggressive course and a poor prognosis. We present three cases of glassy cell carcinoma of the cervix. Patients presented with a cervical growth which was biopsied. Histology the tumours showed nests of cells with a granular or clear cytoplasm, displaying marked pleomorphism and mitoses. Stroma showed an eosinophilic infiltrate. Two tumours showed a pure glassy cell pattern and one showed glandular differentiation with intracellular and extracellular mucin. Patients were treated with a combination of surgery, radiotherapy and chemotherapy but showed a poor response. Two patients died of the disease of pelvic or distant metastases within two years of diagnosis and one was lost to follow up. Although glassy cell carcinoma runs an aggressive clinical course, an early diagnosis may help in a more effective management and offer a better prognosis. Keywords: Cervical neoplasm, Glassy cell carcinoma INTRODUCTION Glassy cell carcinoma (GCC) is an uncommon cervical neoplasm with a characteristic histology. It is a poorly differentiated variant of adenosquamous carcinoma,[1],[2] and shows either an undifferentiated pattern of pure glassy cells or a squamous or glandular differentiation.[2] GCC runs an aggressive course despite a combination of radical surgery, chemotherapy and radiotherapy and the disease is already at an advanced stage at the time of diagnosis. Patients should be evaluated thoroughly for the presence of disseminated disease before starting definitive treatment.CASES Three cases of GCC were diagnosed in our department over a ten year period. Patients were aged between 39- 45 years and presented with vaginal discharge and/or abnormal vaginal bleeding of short duration (2-3 months). The diagnosis was made on biopsy, and patients were treated with combined surgery/ chemotherapy/ radiotherapy [Table - 1]. Gross findings Histologic findings DISCUSSION Glassy cell carcinoma of the uterine cervix is an uncommon, aggressive neoplasm having an incidence of 1-5.75% of all malignant cervical neoplasms,[1],[3],[4] The mean age of patients is about 10 years younger than conventional carcinomas of the cervix.[2],[3] The tumour presents as an ulcerated or non-ulcerated growth around the squamo-columnar junction or grows into the endocervical canal in a barrel-shaped fashion with extension into the vagina and parametrium.[2],[3],[4] It also presents as a cervical polyp, or as a microinvasive lesion.[6],[7] Despite a large tumour volume the cervical stroma is generally involved only superficially.[1],[3] In one of our patients with Stage IB 1 disease the cervical stroma was superficially involved (12 mm), and in both others it was involved upto a depth of 4 mm. with invasion of the adjacent myometrium. In one of our patients with IIIB disease, 2 of 30 pelvic lymph nodes were positive for metastases but in both others, the nodes were negative. Sections show cells are arranged in nests and cords separated by fibrovascular septa. The cells are polygonal with a moderate amount of granular, pale eosinophilic, ground glass cytoplasm and a distinct cell membrane stained well by PAS stain. The cells have an average diameter of 50µ and a nuclear-cytoplasmic ratio of 1:2-3.[1],[2] The nuclei are large, round to oval, with multinucleation and prominent multiple nucleoli.[4],[6] Cellular pleomorphism, numerous abnormal mitoses (about 5/- HPF) spindled bizarre cells and foci of necrosis are usual features.[2] A striking feature of the stroma is a rich cellular infiltrate consisting predominantly of eosinophils, plasma cells and sometimes neutrophils, often infiltrating nests of neoplastic cells.[2],[6] The tumour shows a pure glassy cell pattern or a tendency towards squamous differentiation with keratinization or poorly formed squamous pearls surrounded by glassy cells, sporadic keratinization or dyskeratosis.[2] Few tumours show a tendency towards glandular differentiation in the form of poorly formed glands lined by glassy cells. Mucin secretion is evident in some cases and is predominantly intracellular in the glassy cell areas and extracellular in the glandular areas.[2],[5] To qualify as a GCC, the glassy cell pattern should constitute at least one third of the tumour.[4],[5] Two of our cases showed a pure glassy cell pattern and one case showed a biphasic pattern (70% glassy cell features) with evidence of glandular differentiation (intraluminal and intracytoplasmic mucin) in 30% of the tumour. Cytology smears of GCC show necrotic debris, proteinaceous material and abundant inflammatory exudate chiefly eosinophils or lymphocytes, amongst which are scattered or syncitial clusters of large malignant cells[8],[9] which show a moderate amount of finely granular cytoplasm, distinct cell membranes, large nuclei and prominent single or multiple nucleoli.[6],[8],[9] Tumour cells are intimately associated with inflam-matory cells forming "granuloepithelial complexes."[8] A high mitotic activity and a few atypical, bizarre, multinucleated cells are seen.[9] Squamous differentiation in the form of well-defined granular cytoplasm, oval nuclei and prominent nucleoli may be seen. On cytology, GCC has to be distinguished from atypical reparative cells and large cell non- keratinizing carcinoma.[8] Non-keratinizing SCC shows a greater degree of squamous differentiation, intercellular bridges, coarse chromatin and intracellular glycogen. It lacks the ground glass cytoplasm, well defined cell borders, prominent nucleoli, high mitotic activity, clumped chromatin and the prominent eosinophilic infiltrate seen in GCC.[2],[3],[7]. GCC may be difficult to distinguish from the rare lymphoepithelioma-like carcinoma of the cervix which shows large, uniform tumour cells in an inflammatory background. However the nuclei are oval and vesicular and the cytoplasm is flocculent and ill-defined. The cells of this tumour lack the glassy cell features and tend to grow singly or in syncitial rather than in cohesive groups. Stroma shows abundant lymphocytes.[7] Large areas of clear cell differentiation are occasionally seen in GCC. These are distinct from clear cell carcinoma (mesonephroid carcinoma) of the cervix. Clear cell carcinoma shows glands or papillary processes and characteristic hobnail cells with the nuclei protruding away from the base of the cell. The cells are smaller than in GCC. GCC is usually at an advanced stage at the time of diagnosis and shows a tendency for pelvic and extrapelvic metastases even when the primary is relatively small. Local recurrence usually occurs at the vaginal apex,[1],[10] and pelvic spread occurs to parametrium, ovaries and para-aortic lymph nodes.[1],[10] Extrapelvic spread includes metastases to the lung, liver, spleen and bone marrow.[2] Risk factors for recurrence are lymphatic invasion, deep stromal invasion and tumour size >3 cms.[10] The anatomic extent of the disease is important to determine the prognosis as surgical staging is often higher than clinical staging. Because of all these factors, GCC follows a more aggressive course and carries a poor prognosis.[2],[3],[6] The five year survival for GCC was variably reported to be between 13-30%. The average survival in some studies was reported to be less than a year,[2],[6] the tumour showing little or no cytologic alteration after radiotherapy.[2] The grim outlook for these patients has been considerably improved with the combination of radical surgery with aggressive radiation therapy and Cisplatin containing chemotherapy with an overall survival of 73%, a disease free survival of 64%.[10] and a five-year survival 80%[3],[4] For Stage I patients the outlook is even better with an overall survival of 86% and a disease free survival of 71% on a follow-up of 28.5 months.[10] REFERENCES
Copyright 2004 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn04017f3.jpg] [cn04017f1.jpg] [cn04017f2.jpg] [cn04017t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}