 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
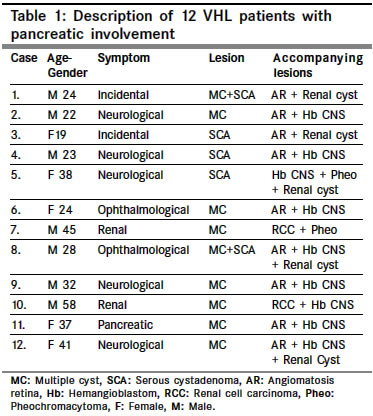
Indian Journal of Cancer, Vol. 41, No. 4, October-December, 2004, pp. 159-161 Original Article Pancreatic involvement in Von Hippel-Lindau disease Eras Mustafa, Yenigun Mustafa, Acar Cengiz, Kumbasar Baki, Sar Fuat, Bilge Turgay Clinics of Neurosurgery, Educational Hospital in Istanbul Code Number: cn04030 ABSTRACT BACKGROUND: Involvement of the pancreas in Von Hippel-Lindau disease that is a tumor predisposing syndrome mentioned in literature with some morbid and mortal progression.AIMS: For evaluation the faith of the pancreatic involvemet in VHL disease we analysed our patient population with VHL disease. MATERIALS AND METHODS: 12 of the 56 patients that were evaluated in our institute with the diagnosis of Von Hippel-Lindau disease had pancreatic involvement. They are periodically examined for 5 years follow up period. Their retrospective analysis was accomplished. RESULTS AND CONCLUSIONS: Pancreatic involvement in our patient population disclosed lesions that were multicysts or serous cystadenomas. During follow up period, we did not observe significant morbidity related to pancreatic involvement. Repeated radiological examination of pancreatic lesions disclosed insignificant modifications such as slight increase or decrease in size. Whereas we considered morbidity and mortality related to renal and central nervous system pathologies in VHL disease. Shortly, even pancratic involvement in VHL disease requires close clinical follow up, morbidity and mortality in this case is not severe as in renal and the central nervous system involvement. Key Words: Von Hippel-Lindau, pancreatic, involvement, cysts, renal cell carcinoma. INTRODUCTION Von Hippel-Lindau (VHL) disease is a tumor predisposing syndrome with autosomal dominant inheritance and affecting one in 36,000 live births annually.[1] Absence of the pVHL that is a multifunctional tumor supressor product of VHL gene identified at chromosome 3p25-26 exposes these patients to origination of different tumors that mainly are central nervous system hemangioblastomas, retinal angiomas, renal cell carcinomas, endolymphatic sac tumors, pancreatic tumors, pheochromocytomas and epididymal cystadenomas.[2],[3],[4] The frequency of pancreatic involvement in VHL disease vary from 17% to 56%,[2],[5],[6] and mainly are cysts, serous cystadenomas, and neuroendocrine tumors (NET), but adenocarcinomas, hemangioblastomas and the renal cell cancer metastasis have also been unusually described.[7],[8],[9] Even pancreatic involvement is relatively benign form of the disease, some morbidity and mortality can be attributed to such lesions via compression of neighbouring structures by huge cysts and metastasis of NET.[10],[11] In this present series, we summarize the pancreatic involvement of 12 well-documented VHL patients and their clinical course during 5 years follow up period. MATERIALS AND METHODS Between April 1989 to April 2003, 56 patients evaluated in our institute with the diagnosis of VHL disease were analysed retrospectively. Determination of the one typical lesion of the disease was enough to establish diagnosis in patients with a first degree relative with VHL disease; whereas in the absence of family history, the determination of at least two VHL lesions including 1 hemangioblastoma of the central nervous system (CNS) or the retina was required for diagnosis. In all of these patients, ophthalmological examination, magnetic resonance imaging of the CNS and either ultrasonography and computerized tomography of whole abdomen with contrast enhancement were performed routinely, and biochemical datas such as serum and urinary peptide levels, serum pancreatic enzyme levels, blood glucose levels were also obtained as needed. Involvement of the pancreas was verified by ultrasonography and computerized tomography with contrast enhanced and detailed examination to describe the pancreatic lesions for such as location, size, number, character, density, calsification; and to describe the peripancreatic region such as main pancreatic duct or biliary duct obstruction, lymph node infiltration and distant metastasis were scheduled. RESULTS Mean age of 56 patients (22 male and 34 female) was 34 years (18 to 72 years). Leading symptoms were neurological symptoms, ophthalmologic symptoms, renal symptoms and pancreatic symptoms in order of frequency, and in two of the patients the diagnosis was incidental during ophthalmological examination. Pancreatic involvement was present in 12 of 56 patients (21.4%) [Table - 1]. The verified involvement in pancreas were the multiple cysts in 9 of the patients, the serous cystadenomas in 5 of the patients and both in 2 of the patients. Any of the patients disclosed the clinical and labaratory findings of the NET and its radiological findings that are well limited, strongly and homogenously enhancing lesion with contrast injection in computerized tomography. The differential diagnosis of the multiple cysts from serous cystadenomas were established according to enhancing pattern considered on computerized tomography. Even the definitive diagnosis could only be made with pathological examination, accurate distinction between these two patologies is not crucial and would be an invasive methods during the follow up period. Septal and peripheral enhancement on computerized tomography are more familiar findings for serous cystadenomas than simple cysts and this criterion was used in differential diagnosis. None of the cystic lesion had radiological features of malignancy such as capsular irregularity or vegetation in its, and there was no evidence of infiltration or metastasis. Average diameters observed for lesions were 32 mm ranging from 4 to 98 mm for cysts, and 69 mm ranging from 18 to 160 mm for serous cystadenomas. In two of the patients peripancreatic involvement were also observed and these were asymptomatic compression of the biliary tract and the duodenum by multiple cysts and serous cystadenoma respectively [Figure - 1]. During the follow up period for five years any of the pancreatic lesions leaded to any morbidity or required surgical intervention. On the other hand two of the patients were lost due to the uncontrollable progression of renal cancer. Repeated radiological examination of pancreatic lesions during follow up period resulted with only insignificant modifications in lesion size such as slight increase or decrease of the size in multiple cysts and serous cystadenomas. DISCUSSION Localization of VHL gene at chromosomal region 3p25-26 in 1988[12] and its isolation in 1993[13] leaded more understanding about the pathological processes appeared in this disease. Different mutational mechanisms leading to inactivation of this tumor suppressing gene, including iatrogenic mutations, loss of heterozygosity with deletion or hypermethylation may cause transmission of this pathology to offsprings via autosomal dominant pattern[14],[15] Most of these tumors seen in VHL patients are multiple or bilateral tending to manifest at young age and threating median life expectancy other than close clinical and radiological follow up. The neurological complications due to cerebellar hemangioblastoma and metastasis of renal cell carcinoma are the outstanding factors incresing mortality in these patients;[7],[16] but advanced diagnostic and theureupatic tools are now becoming the best preventive measures in these patients. The pancreatic involvement in VHL disease mainly pointed as 50% (2,5) and are mainly cystic masses such as simple cysts or serous cystadenomas and the NETs. Complications to the cystic lesions may arise from mass effect causing pain, biliary obstruction, pancreatitis or pancreatic hormonal insufficiency[17],[18] but usually are asymptomatic and rarely necessitate surgical intervention. In our series asymptomatic compression of the biliary tract and the duodenum in two of the patients by multiple cysts and serous cystadenoma respectively did not necessitate any complication during follow up period. Additionally, we did not observe significant increase in size of the lesions during this period. Frequency of NET in VHL disease reported as 20% in the literature.[5],[19] NET more than 3 cm in diameter are impressed as highly aggressive for invasion of the peripheral structures as duodenum, lymph nodes and the liver and metastatic progression has been shown to occur in 25% of cases.[7],[19],[20] The potential malignancy of such tumors recommends the resection of these tumors whenever its possible. We did not diagnose NET in our patient population. In this limited series of the VHL patients with pancreatic involvement, we did not observe any dissapointment due to a pancreatic lesion whereas 2 of our patients were lost due to renal cancer and we needed surgical interventions in some extent for CNS hemangioblastomas we encountered. In summary, pancreatic involvement is not rarely encountered in patients with VHL disease but major challenging part of the disease is treatment of the renal and the CNS pathologies in these patient population. REFERENCES
Copyright 2004 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn04030f1.jpg] [cn04030t1.jpg] |
| |||||||||

{kind=link}
{kind=link}