 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
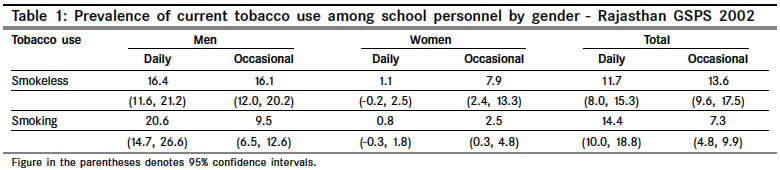
Indian Journal of Cancer, Vol. 41, No. 4, October-December, 2004, pp. 162-166 Original Article Tobacco use among school personnel in Rajasthan, India Sharma Rameshwar, Pednekar MangeshS, Rehman AU, Gupta Rakesh Healis, Sekhsaria Institute of Public Helath, Navi Mumbai Code Number: cn04031 ABSTRACT BACKGROUND: A very little information about tobacco use among school personnel is available. This is a step to have cross country and within country data using standardized methodology. AIMS: To obtain baseline information about tobacco use prevalence, knowledge and attitude among school personnel.STUDY DESIGN: Two stage cluster sample. SETTING: A state of Rajasthan. MATERIALS AND MATERIALS AND METHODS: A cross-sectional study, using anonymous self-administered questionnaire. A sample of schools with probability proportional to the enrolment in grades 8–10. All school personnel in sampled schools were eligible to participate. STATISTICAL ANALYSIS: Percentage, 95% confidence interval. RESULTS: School response rate was 97.4% (75/77) and school personnel response rate was 67.2% (909/1352). Majority of school personnel (men 69%, women 31%) were school teachers (78.3%). The prevalence of ever any tobacco use was reported by 35.9%, more among men than women (46.2% vs. 13.0%). The prevalence of current daily smoking was reported by 14.4% (men 20.6%, women 0.8%) and occasional by 7.3%, where as current daily smokeless tobacco use was 11.7% (men 16.4%, women 1.1%) and occasional 13.6%. Current daily tobacco use was significantly more among men than women. Four out of nine reported their schools have a tobacco prohibiting policy for both students (48.4%) as well as for school personnel (44.4%) and about same (47.2%) reported their schools enforce its tobacco policy or rule. Over 85% of all school personnel strongly support the tobacco control policies and wanted training in tobacco cessation and prevention. CONCLUSION: First study from Rajasthan to report tobacco use among school personnel. School personnel not only strongly support the tobacco control policies but also ready to work for its successful implementation with proper training. Key Words: Personnel, adolescents, policy, daily. INTRODUCTION For adolescent, school personnel form important role models. Recent estimates indicate that between 81000 and 98000 children and young people take up smoking per day worldwide, majority in middle- and low- income countries.[1] Tobacco users often take up use in their teens[2],[3] and the risks of tobacco use are highest among those who start smoking early and continue for prolonged period.[4] As school personnel can potentially influence students′ tobacco use, to plan effective interventions, it is essential to have information on the extent and the type of tobacco use among school personnel, their attitudes towards tobacco control, and the existence of school health polices about tobacco.[5] Tobacco use among 13-15 year old students is being studied worldwide through the Global Youth Tobacco Survey (GYTS).[6] The Global School Personnel Survey (GSPS) is carried out in the same schools at the same time as GYTS. The objectives of GSPS are: (1) to obtain baseline information on tobacco use; (2) to evaluate the existence, implementation, and enforcement of tobacco control policies in schools; (3) to understand the knowledge and attitudes towards tobacco control policies; (4) to assess training and material requirements for implementing tobacco prevention and control interventions; and (5) to verify some information obtained from the GYTS. GSPS reports showed high prevalence of tobacco use in school personnel from Bihar and in eight North-eastern states of India.[7],[8] This document is the first report of school personnel from Rajasthan, India. The state of Rajasthan came into existence on 1st November 1956, when the states of the Indian union were reorganized along linguistic lines. Rajasthan is geographically located between latitude 27.0 N and longitude 74.0 E, covering a population of 56,473,122 (29,381,657 men, 27,091,465 women) at a decadal growth rate of 28.3%. The sex ratio (i.e., the number of females per thousand males) of population in the state has improved from 910 in 1991 census to 921 in 2001 census. The literacy rate has increased to 61.0% (76.5% men, 44.3% women) compared to 38.6% during 1991 census.[9] In the National Family Health Survey (NFHS-2), the prevalence of tobacco use was reported to be high in this part of India.[10] MATERIALS AND METHODS The study was carried out in 2002. GSPS was conducted in the same schools and by same survey personnel selected for GYTS. The schools were sampled with probability of selection proportional to the school enrolment size in grades 8-10 (corresponding to ages 13-15 years). At the first stage, a fixed number of 77 schools were selected with a probability proportional to enrollment size. All school personnel (including non-teaching staff) in the selected schools were eligible to participate. In India, education is a state responsibility and almost all schools were part of state educational system. The questionnaire was self-administered with no identification information collected (name, school or village/ town), maintaining complete anonymity. School personnel completed the self-administered questionnaire during the break hours, recording their responses directly on a sheet, which could subsequently be optically read by machine. All questions required answering (i.e. there was no skipping or branching pattern). This questionnaire was already used in different states[7],[8] and was pre-tested for use in Rajasthan. The tobacco use was mainly classified in two categories: smoking and smokeless. Tobacco was mainly smoked in the form of cigarette and bidi (tobacco rolled in tendu leaf). Smokeless tobacco use in the form betel quid, gutka (industrially manufactured tobacco product, contains areca nut, tobacco and other ingredients), khaini, and snuff which are also common in different parts of India, has been described elsewhere.[11] Data analysis was performed using SUDAAN ® and the C-sample procedure in Epi-Info taking the probabilities of selection into account as well as adjustment for non-response at the school, and school personnel level. Ninety-five percent confidence intervals were calculated and used to test for significance of difference. Whenever a denominator was less than 35, the data were not included in the table. RESULTS Out of 77 sampled schools 75 participated in the survey (response rate 97.4%). The school personnel response rate was 67.2% (out of 1352 sampled); the reason for non-response was absence from school on the day of the survey. Out of the total 909 participating school personnel 69.0% were men; 61.7% were less than 40 years old; and, 14.6% were 50 years or older. Very few (1%) were more than 60 as mandatory retirement age is 60 years. Age distribution was similar in both men as well women. Most of the school personnel were teachers (78.3%) and 2.2% were health personnel. (These results were not shown in the tables) Ever any tobacco use was reported by 35.9% (men 46.2%, women 13.0%), of which ever smoking was 29.6% (men 38.9%, women 8.8%) and ever smokeless tobacco use was 25.4% (men 32.6%, women 9.5%). Current daily smoking was reported by 14.4% (men 20.6%, women 0.8%) while current occasional smoking by 7.3% (men 9.5%, women 2.5%). Current daily smokeless tobacco use was reported by 11.7% (men 16.4%, women 1.1%) while current occasional by 13.6% (men 16.1%, women 7.9%). Current daily tobacco use was reported significantly more among men than women [Table - 1]. Among current smokers (men 95%), 34.2% reported cigarette smoking, 19.5% bidi smoking, 37.3% combination or other forms of smoking. Among men, the most popular form of smokeless tobacco use was gutka (33.3%) followed by betel quid (17.9%) and khaini (17.3%). Among women, gutka (54.3%) and betel quid (21.1%) were commonest. (These results were not shown in the tables) Both ever (42.2%) and never (55.3%) tobacco users considered tobacco was addictive. Overall three-fourth admitted that tobacco use causes serious diseases like cancer (78.4%) and four-fifth believed that environmental tobacco smoke (ETS, 84.0%) was harmful, but it was significantly more by never tobacco users than ever tobacco users. [Table - 2] Four out of nine school personnel reported that there was policy on prohibiting tobacco use, for students (48.4%) as well as for school personnel (44.4%) and about same (47.2%) reported that their school enforces its tobacco policy or rule. About one-fifth of school personnel reported class-room teaching on short-term health consequences (21.0%) and two-third on long-term health consequences (67.9%) of tobacco use. Over half the school personnel were aware and discussed with their students about various issues on tobacco like; how many young people in community or country use tobacco (56.9%), social and cultural influences on tobacco use (58.8%), communication skills (57.5%) and goal setting skills (57.4%) to avoid tobacco use, to resist peer pressure to use tobacco (52.6%). In contrast, training among school personnel to prevent tobacco use (10.5%) and access to teaching material (18.7%) was very limited. However 86.1% school personnel felt need for such training. [Table - 2] Around five out of six school personnel expressed need for a policy prohibiting tobacco use by students (87.3%) and by school personnel (85.7%). Some 83.1% thought that tobacco companies deliberately encourage youth to use tobacco while 80.2% were in favor of not allowing tobacco companies to sponsor sports events. On the other hand, 91.2% wanted a complete ban on tobacco advertisements and 61.2% were in favor of increasing the prices of tobacco products. [Table - 2] DISCUSSION GSPS was the unique study for within-country comparison of tobacco use prevalence, knowledge, attitude among school personnel in India. Given that school personnel play an important role model for children, they could also play very important role in tobacco control efforts as the majority of tobacco users take up use in their teens.[2],[3] Tobacco use was reported among school personnel in Rajasthan. A NFHS-2 household survey of members′ age 15 year and above, conducted in Rajasthan, reported 23.2% ever tobacco use.[10] GSPS Rajasthan also reported similar ever tobacco use (29.6%), but it was reported twice (8.8% vs. 4.4%) among women. The current (daily plus occasional) smoking among men (GSPS, 30.1% and NHFS-2, 37.9%) and women (GSPS, 3.3% and NHFS-2 4.3%) was similar in both studies. Other GSPS studies conducted in different parts of India reported current smoking among men ranged from 79.5% (Manipur) to 45.2% (Arunachal Pradesh) and among women 76.2% (Mizoram) to 9.2% (Tripura).[7],[8] As most of the studies reported from India, cigarette or bidi smoking was the most preferred type of smoking[7],[8],[11],[12],[13] and this was also true in GSPS Rajasthan. In NHFS-2, current chewing among men was 19.1% and among women 3.9%,[10] while GSPS reported current chewing (daily plus occasional) among men 32.5% and among women 9.0%. There is a considerable increased in chewing habits among both men and women. Gutka use could be one of the reasons, as gutka was the most preferred type of chewing tobacco product among men (33.3%) as well as among women (54.3%) in Rajasthan. Gutka is heavily marketed and advertised all over India[14],[15] and is a preferred tobacco product,[7],[8],[13] even among school children.[14],[15] Like many other studies in India,[8],[11],[12] betel quid was also preferred type of chewing tobacco in Rajasthan. The prevalence of former tobacco users is an index of levels of quitting within a population. In high-income countries, former smoker rates have increased over the past two to three decades, and today it ranges from 19% (Spain) to 41% (Sweden) of the men population are former smokers. In contrast, only 2% of Chinese men surveyed in 1993; 5% of Indian men surveyed around same period; and only 10% Vietnamese men had quit in 1997.[1] In GSPS Rajasthan, the prevalence of former men smokers was 8.8%, confirming the pattern and showing a need for support of tobacco cessation. School personnel responding to the GSPS were generally knowledgeable of health hazard of tobacco. Over half the school personnel thought tobacco was addictive, while three-fourth to four-fifth thought tobacco causes serious diseases like cancer and environmental tobacco smoke was harmful. Similar results were reported from GSPS studies conducted in other parts of India.[7],[8] This knowledge has to be supported with proper training and access to teaching and learning material about tobacco use and how to prevent its use. The experience all over the world is that anti-tobacco education is an effective means of stopping or curtailing tobacco use. An intervention study showed that 9-17% of people stopped tobacco use and 20-49% reduced their habit substantially after five years of health education.[18] Even school children who received health education on tobacco and intervention methods were instrumental in achieving stoppage rate of 9.7% among adults. Furthermore, health education imparted a negative attitude to tobacco among the children.[19] The current study reported no training and no learning material was available, but over 85% school personnel expressed need for such training. Similar results were reported from other GSPS studies.[8] Like other states of India,[8] the current study indicated that school personnel were highly concerned about tobacco use among youth in the community, and feels school personnel should set good example by not using tobacco, but, this concern did not translate into actual teaching about tobacco use prevention. Two-fifth of school personnel reported schools in Rajasthan have a policy specifically prohibiting tobacco use among students as well as among school personnel and they also prohibit the use of tobacco by staff, visitors, and students in all buildings, on the grounds, and at school sponsored events. Over half reported their schools enforce its tobacco policy or rule. For effective tobacco control, school personnel opined that tobacco company should not be allowed to sponsor sporting events as they deliberately advertise and promote tobacco products to encourage youth to use tobacco. They strongly support tobacco ban in the state and were in favor of increasing prices of tobacco products. Thus there is a strong support for tobacco control policies in Rajasthan and there are some policies in schools, it appears that effective implementation is lacking. Over all it seems that the school personnel of Rajasthan were concerned about youth and they supported formulation and implementation of tobacco control policies. The effective implementation of policies that would received support from all quarters would be a complete ban on tobacco use inside the school premises by school personnel as well students, ban on sponsorship of any event by tobacco companies that involves and appeals to youth, and increase in price of tobacco products. A public health effort for controlling tobacco use involves; scientific information, public policy, mass media, social marketing techniques and community-based programmes to effect change. No single intervention or just making laws or policies will stop the tobacco epidemic. Public health activities for controlling tobacco use need continuous assessment and evaluation; as successful strategies emerge, they should be adapted to different cultural and social environments. ACKNOWLEDGEMENTS Authors wish to acknowledge the contribution and help from Dr. P. C. Gupta, Director, Healis, Sekhsaria Institute of Public Health, Navi Mumbai, India, Dr. Samira Asma, Associate Director, Charles Warren, Distinguished Fellow, Office on smoking and health, CDC and Dr. Leanne Riley, TFI, WHO. REFERENCES
Copyright 2004 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn04031t2.jpg] [cn04031t1.jpg] |
| |||||||||

{kind=link}
{kind=link}