 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
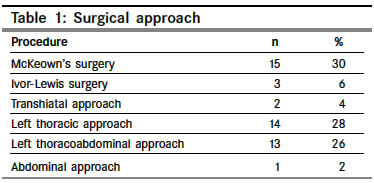
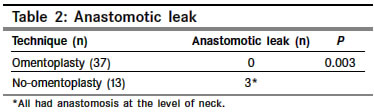
Indian Journal of Cancer, Vol. 41, No. 4, October-December, 2004, pp. 167-169 Original Article Omentoplasty versus no omentoplasty for esophagogastrostomy after surgery for cancer of cardia and esophagus Thakur Binay, Zhang Chun Shan, Tan Zhen Bo Department of Surgical Oncology, BP Koirala Memorial Hospital, Bharatpur Code Number: cn04032 ABSTRACT BACKGROUND: The standard of care of patients with cancer of cardia and esophagus still remains surgery in early stage. One of the most feared complications after such procedure is anastomotic leak.AIM: We present our experience with omental wrapping of anastomosis (omentoplasty) to decrease the anastomotic leak. SETTINGS AND DESIGN:Retrospective study. MATERIALS AND METHODS: An analysis of 50 consecutive patients, who underwent surgical resection for cancer of cardia and esophagus at BPKMCH, is done. For cancer of esophagus, a 10 cm proximal tumor free margin and for lesions of cardia, at least 5 cm margin was achieved. A 5 cm distal tumor free margin was achieved in each case. A subset of patients was considered for omentoplasty after completion of anastomosis. RESULTS: There were 29 male and 21 female with a mean age of 56.3 years. The average postoperative stay was 13.14 days. The stomach was the organ of substitute in 48 and jejunum in 2 cases. Omentoplasty was done in 37 cases, whereas in 13 cases, no omental wrapping was done. The rate of anastomotic leak was 6%. There was no leak from anastomosis placed at chest, whereas three cases of leak was observed in the anastomosis at the level of neck ( P=.013). Overall, there was no leak in omentoplasty group, whereas there were three cases with leak in the group without omentoplasty ( P=0.003). CONCLUSION: Omentoplasty should be considered in every case after surgical resection for cancer of cardia and esophagus. Key Words: Cancer of cardia and esophagus; esophagectomy; omentoplasty. INTRODUCTION The standard of care of patients with cancer of cardia and esophagus still remains surgery in early stage. Different approaches varying from transthoracic to transhiatal and in some cases only abdominal approach have been recommended. Each approach has its pros and cons. One of the most important points in each approach is to reduce the rate of anastomotic leak. If the anastomotic leak occurs in thoracic cavity, it often proves fatal. Main emphasis goes on the meticulous technique of anastomosis without any tension and good vascularity of the substitute. Omental wrapping (omentoplasty) of the anastomotic site, located at thorax has been well accepted method of lowering the chance of leak.[1] Recently several authors routinely recommend this technique even for the anastomosis placed at neck.[2],[3] In this article, we have tried to show our experience with this technique. MATERIALS AND METHODS A retrospective analysis of 50 consecutive patients, who underwent surgical resection for cancer of cardia and esophagus at BP Koirala Memorial Cancer Hospital (BPKMCH), is done. The surgical approach depended upon the location of tumor. For cancer of esophagus, a 10 cm proximal tumor free margin and for lesions of cardia, at least 5 cm margin was achieved. A 5 cm distal tumor free margin was achieved in each case. In transthoracic approach, a two-field lymph node dissection was routinely performed. In all cases, hand sewn two-layered anastomosis was performed with interrupted 000 silk. A subset of patients was considered for omental wrapping after completion of anastomosis. A tongue of omentum along greater curvature of stomach, measuring approximately 4x6 cm was taken along with its vessels preserved and sutured to anterior circumference of anastomosis. Therefore, omentoplasty was only feasible when stomach was used as a substitute. All the patients with the anastomosis at chest (except those who had jejunum as a substitute organ and one case with stomach as a substitute organ) were considered for omentoplasty. For the anastomosis at the level of neck, omentoplasty was taken as a routine policy since year 2004 with the exceptions in few cases, where it was not considered because of technical difficulties. Before year 2004, for the anastomosis at the level of neck, it was considered only occasionally. In left sided transthoracic approach and solitary abdominal approach, a routine per nasal feeding tube was inserted. In other cases, a feeding jejunostomy was put. Feeding through the tube was started on 3rd-4th post operative day, and it was continued in the cases of anastomotic leak till the later healed. A dilute barium swallow was done on 7th postoperative day, and if there was no radiological evidence of leak, oral feeding was started. In a minority of patients with the anastomosis at neck and negative barium study, the leak was diagnosed on clinical grounds once oral feeding was started. Patients were analyzed for age, sex, procedures, rate of anastomotic leak for patients with and without omentoplasty. The statistical analysis was done using SPSS version 10.0. RESULTS Fifty consecutive patients with the diagnosis of cancer of cardia and esophagus were taken for surgery. There were 29 male (58%) and 21 female (42%). The mean age was 56.3 years (range: 36-82 years). The average loss of weight was 8 kg in last 3 months. The average postoperative stay was 13.14 days. The stomach was the organ of substitute in 48 (96%) and jejunum in 2 (4%) of cases. The later cases underwent total gastrectomy with distal esophagectomy, and intrathoracic esophagojejunostomy was performed. These cases were included in no-omentoplasty group. The procedures performed and anastomotic leak have been shown in [Table - 1] and [Table - 2], respectively. There were two in-hospital mortalities (4%), one in omentoplasty group and one in no-omentoplasty group (P=0.51). The rate of anastomotic leak was 6%. There was no leak from 33 anastomoses placed at chest (omentoplasty group=30, no-omentoplasty group=3), whereas three cases of leak was observed in the anastomosis at the level of neck (P=0.013). Overall, there was no leakage in omentoplasty group, whereas all three cases of leakage occurred in the group without omentoplasty (P=0.003). The neck anastomosis was analyzed separately. There were 17 cases where the anastomosis was placed at neck. In seven cases, omentoplasty was done. There was no leak in this group, whereas three cases of anastomotic leak were observed out of ten cases, where omentoplasty was not used. But this value was not significant (P=0.110). All the later cases had microscopically negative (tumor free) proximal margin. DISCUSSION Anastomotic leak is a feared complication in the surgery of cancer of cardia and esophagus because of its high morbidity and mortality. A review of reports in 1980′s by Muller et al revealed an average leakage rate of 12%, and even after that leakage rates of up to 30% were still reported.[4],[5] The risk of leakage from cervical anastomosis is higher than intrathoracic anastomosis. As shown in Muller′s review, it was 11% for intrathoracic anastomosis compared with 19% for cervical anastomosis.[4] But recent series have shown leak rates of 6-8% for cervical anastomosis, and 0 to 2% for intrathoracic anastomosis.[6],[7],[8] If the leak happens in the neck, it can virtually always be dealt with success, but the leak from an anastomosis at chest is usually fatal. Therefore, there are numerous recommendations to avoid this condition, the important ones being - gentle handling to avoid anastomotic site haematoma, meticulous technique of suturing, good vascular supply, tensionless anastomosis and omental wrapping. Omentum has been long used for different purposes for its capacity of localizing infection and sealing micro perforations. In thoracic surgery the omentum is used most widely for the filling of so-called dead spaces at chronic empyema, mediastinitis, chest-wall defects after resection and to strengthen a main bronchus stump in case of a failure after pneumonectomy.[9],[10],[11] It is believed that covering an anastomosis, particularly the one at high risk of dehiscence (e.g., after preoperative radiotherapy), with a well vascularized flap of omentum provides oxygen and nutrients for improved healing. Moreover, the omentum delivers vascular endothelial growth factor, a potent angiogenic factor.[12] This substance appears to be responsible for demonstrated ability of omentum to accelerate neovascularization across anastomotic line.[13] Morgan and colleagues[13] demonstrated revascularization of totally ischemic bronchial autografts with omental flaps in dogs. Most of the authors recommend omentoplasty of anastomosis placed at chest after surgery for esophagus and cardia.[1] There are only few series documenting its efficacy in protecting the anastomotic leak when the anastomosis is placed at neck.[2],[3] Shrager and colleagues retrospectively reviewed 85 cases after complex cardiothoracic procedures where omentoplasty was used.[14] The authors used omentum for prophylaxis of anastomotic dehiscence, established infection and for chest wall resection. There were seven cases of cervical exentration and pharygoesophageal anastomosis, added by omentoplasty. All of them were considered to be at high risk of anastomotic dehiscence because of preoperative radiation or recent chemotherapy/ steroid use. There was no anastomotic leak. Authors concluded that omental transposition should be considered in complex cardiothoracic surgical problems. Ohwada and colleagues reported the anastomotic leakage rate of 2.1% vs. 20% (P<0.01) for omentoplasty (n=48) and no-omentoplasty (n=15), respectively for cervical esophagogastrostomy after radical esophagectomy.[2] Same authors had earlier reported a leakage rate of 3.1% in 32 patients with cancer of esophagus, who underwent radical esophagectomy with three-field lymph node dissection and cervical esophagogastrostomy with omentoplasty.[3] Our series very well shows that there was no leak in 37 cases where omentoplasty was used. Though there was not a significant difference irrespective of omentoplasty when the anastomosis was placed at neck, we think the later finding could be because of small sample size. The process of omental wrapping in itself is very simple and hardly takes more than 7-8 minutes of extra time. Therefore, in conclusion, we strongly recommend omentoplasty in every case of radical surgery for cancer of cardia and esophagus to minimize the anastomotic leak. REFERENCES
Copyright 2004 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn04032t1.jpg] [cn04032t2.jpg] |
| |||||||||

{kind=link}
{kind=link}