 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
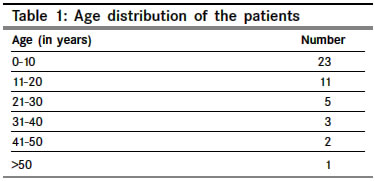
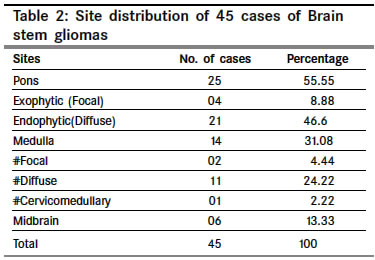
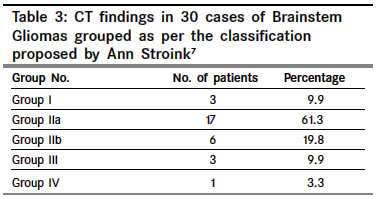
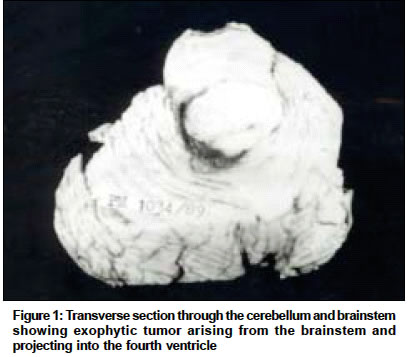
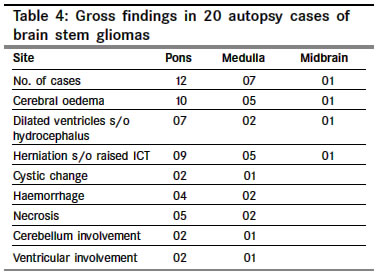
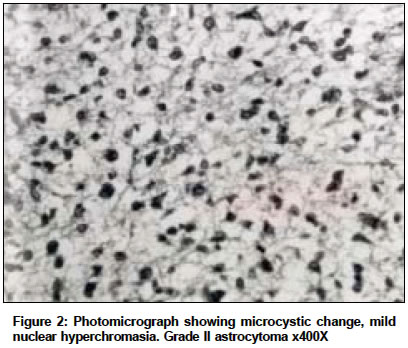
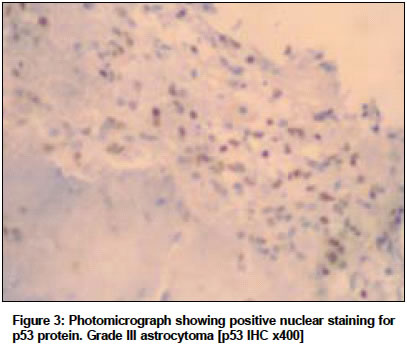
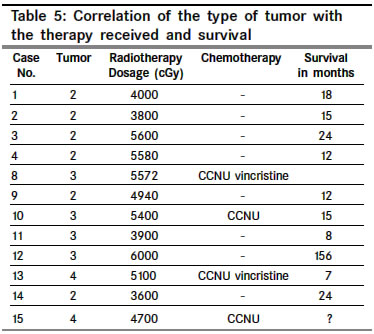
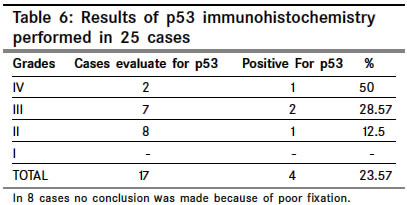
Indian Journal of Cancer, Vol. 41, No. 4, October-December, 2004, pp. 170-174 Original Article Brainstem gliomas – A clinicopathological study of 45 cases with p53 immunohistochemistry Badhe PrernaB, Chauhan PritikaP, Mehta NishakiK Departments of Pathology, Seth G. S. Medical College and KEM Hospital, Parel, Mumbai Code Number: cn04033 ABSTRACT BACKGROUND: Brainstem tumors represent 10% of central nervous system tumors, accounting for 30% of pediatric posterior fossa tumors.AIMS: The aim of this study was to clinicopathologically correlate 45 cases of brain stem gliomas and determine the occurrence and prognostic significance of p53 expression. MATERIALS AND METHOD:45 cases of brain stem gliomas encountered during a 19-year period. 30 were diagnosed by surgical biopsy and 15 at autopsy. In 25 cases p53 immunohistochemistry (Avidin Biotinylated technique) was performed. The WHO brain tumor classification and Stroink’s CT classification were applied. STATISTICAL ANALYSIS USED: Chi square test. RESULTS AND CONCLUSIONS: 51 % of gliomas were observed in the first decade of life. The female to male ratio was 1.04: 1. The commonest presenting features were cranial nerve palsies (33%) and cerebellar signs (29.8%). 55.55% of cases were located in the pons, 31.01% in the medulla and 13.33% in the midbrain. Diffuse astrocytomas were seen in 40 cases (5% were Grade I, 47.5%Grade II, 32.5% Grade III and 15% Grade IV) and pilocytic astrocytomas in 5 cases. Grade IV patients had 2- 3 mitoses /10 high power fields and had a poorer survival rate. Grade II astrocytomas were treated with excision and radiotherapy, while grade III and IV tumors were treated with radiotherapy and chemotherapy (CCNU). Improvement was noted in 20% of patients postoperatively. The outcome was better in patients who were treated surgically. p53 is a frequently mutated gene in brain stem astrocytomas. It was found in 50 % of glioblastoma multiforme, 28.57% of grade III astrocytoma and 12.5% of grade II astrocytoma, while grade 1 astrocytomas failed to express p53 protein. p53 positivity was more in high grade lesions, decreasing significantly in lower grade lesions. Key Words: p53, brainstem, astrocytoma, glioblastoma multiforme, pons, midbrain, medulla, gliomas. INTRODUCTION Brain stem gliomas are a heterogeneous group of tumors commonly seen in children. They represent approximately 10% of the tumors arising in the central nervous system and 30% of paediatric posterior fossa tumors.[1],[2] Those localized in the midbrain (7 to 8%) are almost always low-grade astrocytomas and are associated with good prognosis, those localized to the medulla (10 to 15%) are also usually low grade astrocytomas with good to fair prognosis, but those localized to the pons (80%) are thought to have a dismal prognosis.[3] Although controversies persist in the diagnosis and treatment of brain stem gliomas, histological studies of the lesion are essential to make a definitive diagnosis and decide on appropriate treatment. Ours being a longitudinal study over a period of 19 years MRI findings were available only in 3 cases thus biopsies remained indispensable to initiate treatment. The reasons to biopsy brainstem gliomas are to diagnose the tumor type especially focal brain stem lesions and to decompress the exophytic tumors.[4],[5],[6] In this study we clinicopathologically correlated 45 cases of brain stem gliomas over a 19-year period. The p53 gene is the most commonly mutated gene in a wide variety of human malignancies and is frequently mutated in astrocytomas, hence p53 immunohistochemistry was also studied to determine its occurrence and prognostic significance in brainstem gliomas. MATERIALS AND METHODS This is a retrospective analysis of 45 cases of brain stem gliomas encountered during a nineteen-year period in the Neuropathology Department, of a large teaching hospital. We defined the brain stem in this study as the mesencephalon, pons and medulla and excluded tumors of the thalamus, the hypothalamus and those, which originated in the cerebellum with extensions into the brainstem. 30 cases were diagnosed by surgical biopsy and the remaining 15 at autopsy. The clinical data and operative findings were obtained from the medical case records of the Neurosurgical Department of the Hospital. The information regarding treatment and follow up was collected from the Cancer Research Institute, Mumbai. Surgical biopsy specimens as well as autopsy brains were fixed in 10% formalin. Autopsy brains were fixed in formalin for four weeks. In autopsy cases four to five sections were taken from the tumor, one section from the cortex and one from the basal ganglia along with the ventricular lining. Biopsies were processed as a whole. Sections obtained were cut at 6-micron thickness and routinely stained with haematoxylin eosin. Special stains were performed like Phosphotungstic Acid Haemotoxylin [PTAH] and Rectic, Glial Fibrillary Acidic Protein [GFAP] when necessary. Immuno histochemical stains for mutant p53 were performed in 25 cases using the Avidin Biotinylated technique at Tata Memorial Hospital, Mumbai using the mouse monoclonal antibody, clone no DO7, lot no 108, in the dilution of 1:50, against human p53 protein which was cultured in E. Coli, with inbuilt controls. RESULTS A total number of 45 histologically verified brain stem gliomas were encountered over a 19-year period. Most cases occurred in the first decade of the life (51%). [Table - 1]. There were 23 females and 22 males. The common clinical features associated with brain stem gliomas included cranial nerve palsies (33%) cerebellar signs (29.8%), weakness of limbs (26.4%), signs of raised intracranial tensions(headache - 20%, papilloedema- 12.2% and hydrocephalus - 6.6%) and altered sensorium (15.6%). Pons was the most common site involved (55.55%) followed by the medulla (31.01%) and the midbrain (13.33%) [Table - 2]. Gliomas were grouped as per the classification proposed by Ann Stroink.[7] The commonest finding was a hypodense nonenhancing intrinsic tumor of the brain stem (61.3%) [Table - 3]. CT scan could not accurately diagnose all brain stem gliomas. 5 patients were misdiagnosed: as tuberculoma (3 cases), infarction (1 case) and abscess (1 case). MRI findings were available in only 3 cases. These showed a large exophytic masses occupying the brainstem region which was isointense on T1 and hyper intense on T2. In 8 of our patients an air ventriculogram was performed, which suggested the diagnosis of glioma. Gross findings at autopsy (including 5 postoperative cases) revealed tumors, which were varied in size from 2 cms to 9 cms, were greyish white lobulated, gelatinous and gliotic, with areas of haemorrhage and necrosis [Figure - 1], [Table - 4]. Tumors were classified according to the WHO classification; 5% were Grade I, 47.5% Grade II, [Figure - 2] 32.5% Grade III [Figure - 3] and 15% Grade IV (Diffuse astrocytomas were seen in 40 cases and pilocytic astrocytomas in 5 cases). The diagnosis of pilocytic astrocytomas was made at autopsies. In our study the only histological feature in the biopsy specimen that was significantly associated with a decreased survival was mitoses. 6 cases of Grade IV astrocytomas showed 2- 3 mitoses per 10 high power fields while 14 cases of grade III astrocytomas had 1-2 mitosis per 10 high power fields. Patients with grade II astrocytomas were treated with excision of the tumor and radiotherapy, while grade III and IV astrocytomas were treated with radiotherapy and chemotherapy (CCNU) [Table - 5]. Of the 25 patients who underwent surgery, four patients were alive for 1-2 years after the surgery, while one was alive 13 years postsurgery. Fifteen patients died of the tumor. Ten patients died within one year of the surgery and the remaining five patients within 3 years of the operation. In five patients follow up could not be obtained. In twenty of our patients, diagnosis was made at autopsy. These patients were admitted to the hospital in poor general condition. They died within 2 days to 3 months of admission. The mutant p53 gene has a longer half-life, which can be detected by p53 IHC for p53 protein. Wild type p53 protein in the normal brain has a short half-life and is not detected by p53 IHC. We could study p53 immunohistochemistry in 25 cases. In 8 cases no conclusion could be arrived at due to poor fixation. p53 protein was found in 50% of glioblastoma multiforme, 28.57% of grade 3 astrocytomas and 12.5% of grade 2 astrocytomas while grade 1 astrocytoma have failed to express p53 protein. In [Table - 6], chi-square test value was close to 0.1 (P value> 0.05) DISCUSSION Epstein F suggested a primary staging system for poor risk and high risk patient populations and this classification was thought to be important in assessing therapeutic options.[8] The histological features associated with the poorest survival time were the presence of mitoses, necrosis, and pleomorphism. We observed mitoses, necrosis, and pleomorphism in 20 cases of (high grade astrocytomas) grade III and IV. Features associated with the best prognosis were Rosenthal fibers and calcification.[9],[10],[11],[12] In our study prognostic value of Rosenthal fibres could not be assessed as these patients were not diagnosed and treated at an early stage, rather they came to the hospital in a very bad condition and died within one week of admission. Artigas et al emphasized the importance of stereotactic biopsies for brainstem gliomas as their outcome depends upon the histological identity of the tumors. Their conclusion was histological examination cannot be replaced by CT or MRI as was seen in our study.[13] Yoshimura J, in a clinicopathological study of 40 autopsy cases of diffuse type brainstem gliomas observed that diffuse type brainstem glioma was one of the most malignant types of brain tumors and the prognosis was extremely poor. The proliferative potential of these tumors was presumed to be very high, but there is little information about the cell kinetics of brainstem glioma as surgical resection is rarely performed.[14] However Chico-Ponce de Leon F in a study of fifty patients with infiltrating tumors of the brainstem felt the need for stereotactic biopsies in order to arrive at a precise diagnosis in environments in which MRI may be unavailable. At present, presumptive diagnosis of infiltrating brainstem lesions may be adequately undertaken with imaging methods, such as MRI. However, he believes that a stereotactically guided biopsy provides an accurate method for diagnosing lesions of the brainstem. In his cases, this procedure had been carried out entirely in the tomography room, without any complications of disease or mortality.[4]. Kansal S, in a study of 111 cases of brain stem gliomas observed that the outcome was better in patients who were treated surgically and that the patients with brainstem glioma could be helped by surgical decompression, followed by adjuvant radiotherapy and chemotherapy.[15] Jallo GI states that tumors arising in the brainstem were once uniformly discounted as surgically unresectable lesions. Early neurosurgeons thought this location to be inoperable and fraught with disaster however with the advent of computed tomography (CT), magnetic resonance imaging (MRI), and sophisticated neurophysiological monitoring techniques have significantly advanced the surgical treatment of these precarious lesions.[16] Ostertag et al had studied the monoclonal antibody Ki-67 as a marker for proliferating cells in stereotactic biopsies of brain tumors. They had studied 52 brain tumors. Among the gliomas, highest fractions of proliferating cells were seen in 2 anaplastic paediatric brain stem gliomas [17.5%] and in an anaplastic ependymoma [12.5%].[17] The p53 gene is the most commonly mutated gene in a wide variety of human malignancies and is frequently mutated gene in astrocytomas. Immunohistochemistry of the p53 protein has been used to screen astrocytomas. Wild type p53 protein has a short lifetime of 20-30 minutes and is expressed at low levels in all normal mammalian cells. The wild type of protein is not generally detectable by immunohistochemistry. Mutant p53 proteins have an extended half-life and can be detected by immunohistochemistry due to their protein accumulation. Positive staining was confined to the tumor cells and was not noted in endothelial cells or the adjacent normal brain. Louis et al observed IHC positivity in 3 of 8 (37.5%) grade II astrocytomas, 7 of 12 (58.33%) grade III astrocytomas and 7 of 14 (50%) GBM. We encountered p53 protein in 50% of glioblastoma multiforme, 28.57% of grade III astrocytoma and 12.5% of grade II astrocytomas while grade 1 astrocytomas failed to express p53 protein. Thus p53 positivity was more in high grade lesions decreasing significantly in lower grade lesions.[18] However as our P value was > 0.05, a larger study is required. Weiss WA observed that few genetic studies exist on pediatric brain tumors, in part because tissue from low-grade and brain stem tumors is not readily available.[19] Further studies are needed to identify genetic alterations in pilocytic and diffuse astrocytomas. ACKNOWLEDGEMENTS We would like to thank Dr. S. K. Pandya, Professor and head of the Neurosurgery Department, Seth G. S. Medical College and KEM hospital for the help rendered during the study. We also express our gratitude to Dr. K. N. Naresh, Tata Memorial Hospital for the immunohistochemistry study. REFERENCES
Copyright 2004 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn04033f1.jpg] [cn04033t4.jpg] [cn04033t1.jpg] [cn04033t2.jpg] [cn04033f3.jpg] [cn04033t5.jpg] [cn04033f2.jpg] [cn04033t3.jpg] [cn04033t6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}