 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
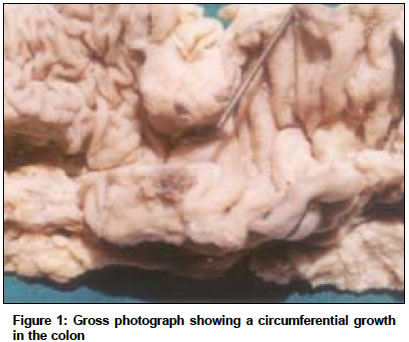
Indian Journal of Cancer, Vol. 41, No. 4, October-December, 2004, pp. 175-177 Case Report Gastrointestinal stromal tumour of the colon presenting with intestinal obstruction Gupta Sanjay, Punia Rajpal Singh, Kaushik Robin Departments of Surgery, Government Medical College and Hospital, Chandigarh Code Number: cn04034 ABSTRACT Gastrointestinal Stromal Tumours are the commonest mesenchymal tumors of the gastrointestinal tract, the stomach and small intestine being the favored sites. They rarely occur in the colon and rectum and esophagus. The diagnosis is difficult, especially in the rarer sites, since there are no pathognomic features to suggest GIST on preoperative clinical examination and investigations, and only a detailed histopathological analysis of the specimen reveals their true nature. The case of a young female patient who presented with intestinal obstruction due a GIST of the transverse colon is reported. The relevant literature is briefly reviewed.Key Words: Intestinal obstruction, GIST, large bowel, colonic tumour, imatinib. INTRODUCTION Gastrointestinal Stromal Tumours (GISTs) are a heterogenous group of mesenchymal tumours that arise from the gastrointestinal tract, and have been the cause of much confusion as to their origin, classification, biological behaviour and prognosis. They have been called by many names such as STUMP (smooth muscle tumours of uncertain malignant potential), GANT (gastrointestinal autonomic nerve tumours), and, GIPACT (gastrointestinal pacemaker cell tumours) in the past. However, advances in immunohistochemistry and electron microscopy have shown that these tumours originate from interstitial cells of Cajal (ICC) or stem cells differentiating towards the ICC.[1] GISTs are currently defined as CD-117 positive (more than 10% tumor cell positivity) spindle cell or epithelioid neoplasms with minimal or incomplete myogenic or neural phenotype.[2] Tumours of true smooth muscle, neural, fibroblastic or vascular origin are not considered in the category of GISTs. We report this rare case of intestinal obstruction due to a transverse colonic tumor that was diagnosed to be a GIST on histopathological examination. CASE REPORT An 18 year old female patient attended the surgical emergency with abdominal pain and distension for a duration of one week. Examination was unremarkable except for the presence of a vague lump in the right iliac fossa. Her routine hematological and biochemical investigations were within normal limits, but since her abdominal x-ray revealed a few air-fluid levels in the ileum, she was managed conservatively as a case of subacute intestinal obstruction with a second possibility of appendicular lump. She remained well for another day, after which she developed low grade fever, with an increase in abdominal distension and the total leukocyte counts. Based on the clinical findings, we decided to explore the patient the very same day. Surgery was performed by a midline incision. There was a large, circumferentially obstructing tumour in the transverse colon, slightly to the left of the midline [Figure - 1]. The proximal large and small bowel was grossly distended and full of fecal matter. There was no evidence of metastasis within the abdominal cavity, and an extended right hemicolectomy was performed, with exteriorization of the proximal end as a stoma in the right lower abdomen. The patient did well in the post-operative period, and was discharged on the 6th day after surgery. Restoration of bowel continuity was performed about 8 weeks later. There was no evidence of the disease during the second surgery, and she remains well on a follow up of 6 months The histopathology report of the tumour revealed GIST of the colon [Figure - 2], with metastasis in 1 out of the 22 lymph nodes resected. DISCUSSION Colonic obstruction usually occurs secondary to colonic adenocarcinoma, but at times, rare tumours may be encountered. GISTs are an extremely rare subset of colonic tumors that are difficult to distinguish grossly from the commonly encountered adenocarcinoma. GISTs are found commonly in the stomach (60 - 70%) and small intestine (20 - 30%), and rarely in the colon and rectum (5 - 10%) and esophagus (less than 5%).[1] When in a colonic location, about two thirds of these GISTs occur in the left or transverse colon.[3] These tumours predominantly occur in middle aged or older persons, the median age at presentation being sixty years, and are uncommon below forty years of age.[1],[4] Males and females are affected equally, but a peculiar subset occurs in female patients below the age of 21 years, either singly or in association with pulmonary chondromas and extra-adrenal paraganglionomas (Carney′s syndrome). Although the malignant potential of colonic GISTs is not certain, upto half are malignant, with a highly aggressive clinical course.[5] Microscopically, GISTs are well-circumscribed smooth lobulated, uncapsulated tumours having a homogenous ′whorled silk′ appearance. They are composed of spindle cells or epithelioid cells, or a mixture of both, and may show areas of cystic degeneration, necrosis or focal hemorrhage.[4],[6] Although they are generally considered malignant, the malignant potential of these tumours is difficult to be determined. It remains difficult to classify them simply into benign and malignant tumors because their biological behaviour remains unpredictable, and the anatomical site of origin, changes of necrosis, hemorrhage, cystic degenerative changes, nuclear atypia, marked cellularity, mitotic rate of above 5 / 50 high power field, or mucosal invasiveness that have been proposed as markers for malignant behaviour, all remain non specific and may be seen in benign tumors as well.[1],[4],[7] Grossly, GISTs may vary greatly in size. Smaller tumours (2 cm or less) are usually asymptomatic and are usually detected incidentally during investigations or at surgery for unrelated pathology. These often exhibit a benign nature, but at times, may present with metastasis to the liver and lungs.[8] Larger tumours usually behave like malignant tumors, and may present with abdominal pain and gastrointestinal bleeding due to ulceration of the overlying mucosa, abdominal mass, or with non-specific symptoms such as weight loss, vomiting, fever and anemia. Depending on the site, the tumor may also present with obstruction, dysphagia, altered bowel habits, or rarely, obstructive jaundice.[7],[9] However, tumour size does not always correlate with malignant behaviour, with smaller tumours being equally capable of metastasis and a clinically aggressive course.[5] The diagnosis of the GISTs is largely histopathological, but may be considered when faced with a large mass without lymphadenopathy at CT scan, or, at laparotomy. Trans-abdominal needle biopsy is not recommended for making a diagnosis in potentially resectable cases because of the risk of tumour seeding.[7] Complete gross excision of the tumor is the treatment of choice.[4],[8] Although there was nodal involvement in our patient, routine lymph node excision is not recommended since they are rarely involved.[4],[7] However, it must be stressed here that in the absence of a clear cut diagnosis of colonic GIST, surgery must proceed as if for adenocarcinoma and radical clearance should be done. Care must be taken to avoid tumour rupture during surgery, since this has been implicated as one of the causes of recurrence.[4] Although radiotherapy and chemotherapy have not been found to be of much help as adjuvant treatment of these tumours, trials are underway to define the role of imatinib (STI 571), a selective and competitive inhibitor of tyrosine kinase, as adjuvant therapy following complete gross excision, as it has been found to be beneficial in the treatment of metastatic and locally advanced GISTs.[4],[10] REFERENCES
Copyright 2004 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn04034f1.jpg] [cn04034f2.jpg] |
| |||||||||

{kind=link}
{kind=link}