 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
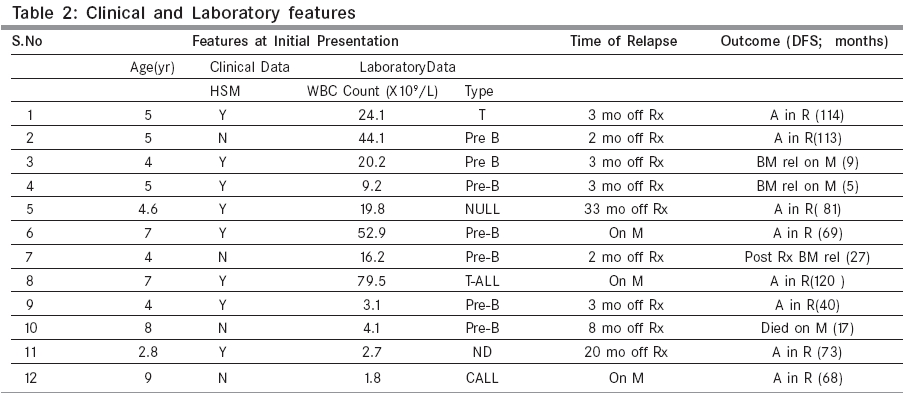
Indian Journal of Cancer, Vol. 42, No. 2, April-June, 2005, pp. 65-69 Original Article Isolated testicular relapse in acute lymphoblastic leukemia - Effective treatment with the modified CCG-112 protocol Shama Goyal, Bhagwat Roshni, Pai SureshK, Kurkure PurnaA, Nair ChandrikaN, Parikh PurvishM, Mukaden MaryannA, Banavali ShripadD Departments of Medical Oncology, Tata Memorial Hospital; Dr. Ernest Borges Road; Parel, Mumbai 400012 Code Number: cn05013 Abstract BACKGROUND: The testes have been considered a sanctuary site for leukemic cells and testicular relapses used to account for a major proportion of the poor outcome of boys with acute lymphoblastic leukemia. With use of aggressive chemotherapy which includes intermediate or high dose methotrexate, the incidence of testicular relapses has declined. However once these patients have received cranial irradiation as a part of the front line protocol, high dose methotrexate needs to be avoided because of risk of developing leucoencephalopathy.AIM: To study the use of non cross resistant chemotherapeutic agents along with a regimen containing lower doses of methotrexate in patients of isolated testicular relapse (ITR). MATERIALS AND METHODS: This is a retrospective analysis of 12 consecutive patients with ITR treated with modified version of the CCG-112 protocol which consists of intensive systemic chemotherapy, cranial chemoprophylaxis along with testicular irradiation. RESULTS: One patient died of regimen related toxicity. Two patients relapsed in the bone marrow during maintenance. Of the nine patients who completed treatment, eight are alive and in remission. One patient had a bone marrow relapse two months after completing treatment. The Kaplan Meier estimates give us an Event Free Survival (EFS) of 66.7% at 10 yrs. CONCLUSIONS: Thus, though the incidence is very low, patients with ITR should be treated aggressively since they have an excellent chance of achieving a long term EFS. Keywords: Childhood acute lymhoblastic leukemia, Modified CCG protocol, Isolated testicular relapse Introduction The testes have since long been considered a sanctuary site for leukemic cells and testicular relapses used to account for a major proportion of the poor outcome of boys compared to girls with acute lymphoblastic leukemia (ALL). With use of aggressive chemotherapy which includes intermediate or high dose methotrexate, the incidence of testicular relapses has declined to 0 to 2.8%. [1],[2],[3] At our centre even without use of intermediate or high dose methotrexate, testicular relapses have significantly reduced to 3.2%.[4] Because of this, the focus has now shifted to the pathogenesis of isolated testicular relapse (ITR) and its impact on survival as compared to relapse at other sites. As more of these boys survive in second remission following salvage chemotherapy, the long term consequences of treatment on puberty and sexual function are likely to become more important in the future. We present here the outcome of a series of 12 such patients who were treated with a modified version of the Children′s Cancer Group (CCG) 112 protocol which combined intensive chemotherapy and local irradiation with cranial chemoprophylaxis.[5] Materials and Methods Between November 1991 and May 1998, 12 patients with ALL in first remission and ITR were registered on this protocol. Patients with previous or concurrent bone marrow relapse were ineligible. All patients had received the MCP 841 protocol for ALL which includes induction with vincristine, daunorubicin, l-asparaginase and prednisolone; central nervous system (CNS) prophylaxis with cranial irradiation and intrathecal methotrexate; repeat induction similar to the first induction; consolidation with cytosine arabinoside, mercaptopurine and daunorubicin, and maintenance upto two years with oral mercaptopurine and methotrexate.[4] Testicular relapse was diagnosed clinically and confirmed by testicular biopsy. Bone marrow (BM) and CNS remission was documented. Clinical remission of overt ITR was documented at the end of induction and was defined as the return of testicular size to normal in a well boy with normal counts and no other symptoms and signs of disease. A second testicular biopsy was not performed in any patient. Treatment: As shown in the [Table - 1], the modified CCG-112 protocol (Regimen B) consisted of induction with vincristine, l-asparginase, daunorubicin, prednisolone and cyclophosphamide along with intrathecal methotrexate. Testicular radiation was given simultaneously with induction chemotherapy. Following induction, all patients received consolidation with vincristine, cytosine arabinoside, thioguanine, l-asparginase and prednisolone with intrathecal as well as intermediate dose methotrexate. Ninety six weeks of maintenance therapy was given in pulses of 8 weeks per cycle upto 12 such cycles. Intrathecal methotrexate was continued once during each maintenance cycle. Drugs used were similar to those used in induction and consolidation with the addition of doxorubicin and thioguanine. Since the maximum tolerable dose of doxorubicin had exceeded 500 mg/m2 by the second maintenance, the patients were given etoposide instead during further maintenance cycles. Testicular radiation: Patients received radiation therapy bilaterally to the testes and inguinal canals given by megavoltage equipment. Both testes were irradiated through a single anterior port encompassing the scrotal skin laterally and inferiorly. The total dose administered was 2400 cGy in eight fractions of 300 cGy each. If testicular enlargement was present after 2400 cGy, the dose to both testes was increased to 3000 cGy using the same fractionation. Statistical methods: Event free survival (EFS) was measured from the date of onset of treatment to the date of relapse, death or last follow up. Probability estimates of EFS were calculated by the method of Kaplan and Meier with standard errors of Peto et al.[6] The analysis of relationship of prognostic features with EFS was however confounded by the small size of study population. Results The study was opened for patient entry from November 1991. The ages of the patients at initial diagnosis of ALL ranged from two years eight months to nine years with a mean age of five years four months. All twelve patients had an overt testicular relapse as evidenced clinically and confirmed histologically on biopsy of the testes. Patient characteristics shown in [Table - 2] reveal that three patients, namely patient numbers six, eight and 12 relapsed prior to completion of maintenance therapy of MCP 841 protocol of ALL. Another six patients experienced a relapse within six months of cessation of this treatment. All patients went into remission following induction and local irradiation to testes. Only three out of 12 patients received a dose of 30 Gy because of persistence of testicular enlargement at the end of 24 Gy. The remaining nine patients received 24 Gy. All patients then went on to complete consolidation and started the maintenance therapy of the protocol. Patient ten developed fever with hepatitis and pneumonia following the eighth maintenance cycle. He succumbed to infection which was probably of fungal etiology. Two patients relapsed in the bone marrow while on maintenance phase of the protocol. They died subsequently. Nine out of 12 patients went on to complete the protocol within the stipulated time of 24 months. Of these, one patient experienced a bone marrow relapse two months after completion of therapy and died. Eight patients are now in second remission following completion of therapy with a disease free period ranging form 40 to 120 months. The median follow up of this group of patients is eight year one month (range two months to 13 yrs). The ten year EFS with this aggressive therapy is 66.7%. [Figure - 1]. All three patients who relapsed while on maintenance phase of the front-line protocol completed therapy successfully and continue to be in remission for 69, 120 and 68 months. Discussion In this study 12 patients with ITR were treated with the modified version of the therapeutic CCG-112 protocol (Regimen B). Of these patients, 75% experienced an ITR prior to or within six months of completion of frontline therapy. Three of the nine patients who relapsed early eventually experienced a second relapse and fared poorly. Of the three patients who relapsed more than 6 months off therapy two are doing well; they are 81 and 73 months off therapy respectively. The third patient died of infection while his disease was in remission. Our study has shown no significant difference in outcome between on therapy and off therapy relapses. This is at variance with observations made by Uderzo et al and others who found off therapy relapses to have a better outcome than on therapy relapses. [7],[8],[9],[10],[11] Our frontline protocol does not contain intermediate dose methotrexate which may partly explain the above finding. Results with salvage therapy may have improved due to incorporation of systemic methotrexate. We report here EFS of 66.7% at ten years with the use of intensive systemic therapy with testicular irradiation and CNS chemoprophylaxis. These results are similar to those reported by Grundy et al[9] who had an event free survival (EFS) of 59% at six years in their group of 33 boys with an ITR. However, our results are slightly different from those of Finklestein et al[5] who have documented a DFS of 43% with the same protocol. This maybe because all their patients were early on therapy relapses who were more likely to have had systemic disease upfront. Also, we have used etoposide instead of doxorubicin during maintenance in our patients which may have improved our results. The pathogenesis of testicular relapse still remains controversial. It was initially believed that testicular relapse results from residual or resistant leukemia at other sites and heralds the onset of systemic disease10. However, this seems unlikely since relapses with testicular involvement appear significantly later than other medullary and extramedullary relapses[12]. It has been now suggested that various intratesticular factors like the endothelium and the interstitium may locally control the penetration and decrease the intratesticular proliferation of leukemic lymphoblasts so that the cytotoxic drugs become ineffective.[12] These dormant cells may eventually proliferate to produce a relapse. It has been suggested that physiological pubertal changes in the permeability of the vascular endothelium and immunosuppressive effect of the testis may be important explanatory factors for the smaller number of testicular relapses in men compared to boys seen after treatment of ALL[13]. Testicular relapses, either isolated or in combination with a medullary relapse do better than isolated medullary or other extra medullary relapses.[12] Whether this is due to local intratesticular regulation of leukemic lymphoblasts is still to be clarified. As these patients continue to be in second remission after salvage therapy, endocrine dysfunction has become a major issue of concern. Grundy et al found that 82% of their survivors required hormonal treatment for induction or continuation of puberty, or both.[9] It is well known that germ cell dysfunction is common even with scattered doses of irradiation to testes. However, Leydig cell function appears relatively resistant to chemotherapy as well as to doses of irradiation as high as 12 Gy. It becomes more likely once the dose increases beyond 12Gy and is inevitable with doses in excess of 20Gy.[9] We are now evaluating the endocrine and sexual function of our survivors since all have received local radiotherapy to testes in doses of 24-30Gy. At last follow-up all patients progressed into puberty spontaneously. Three out of the eight patients who had a hormonal profile done had elevated luteinizing hormone and decreased testosterone indicating gonadal dysfunction. Of these two are on testosterone replacement therapy. The role of intermediate dose methotrexate in decreasing incidence of testicular relapse has been long known[14] and is further substantiated by the recent St Jude and BFM studies.[1], [3] Therefore it is to be reinforced that intermediate dose methotrexate needs to be incorporated more and more as front-line prophylaxis for testicular relapses. In the past early testicular biopsy in males with ALL was undertaken to detect occult testicular relapses. However it was later abandoned since it did not make an impact on subsequent event free survival.[15] Instead careful and minute clinical examination of the testicles, estimating their size and consistency should be performed regularly at short intervals. In conclusion, this paper shows evidence that boys with ALL having ITR still have good chance of long term EFS and should be aggressively treated. Though the numbers are small, our data also shows that the outcome of ITR is good even for patients who have relapsed on-treatment. However, these boys who survive in second remission need close follow-up so as to facilitate appropriate intervention to avert pubertal delay. Since many of the patients in India are treated on the MCP 841 protocol, modified CCG - 112 may be an effective protocol for relapsed patients. References
Copyright 2005 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn05013t2.jpg] [cn05013t1.jpg] [cn05013f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}