 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
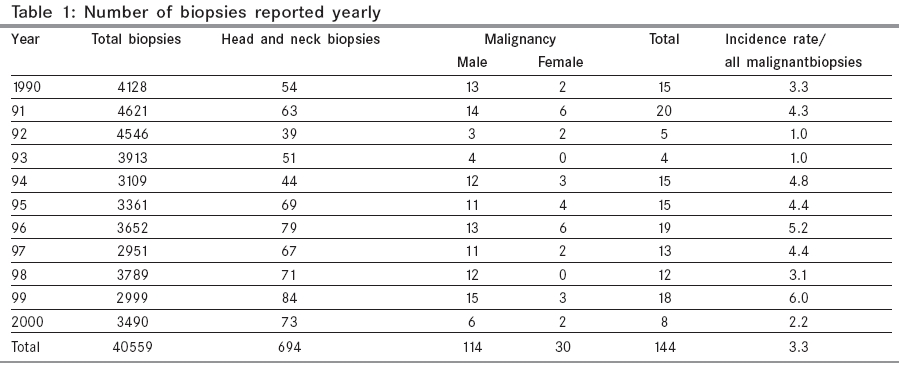
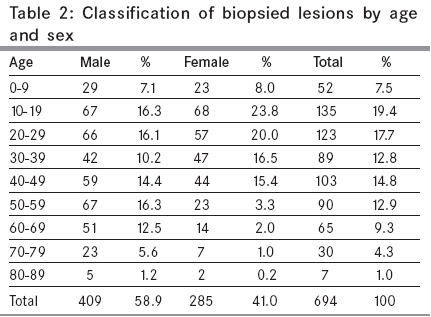
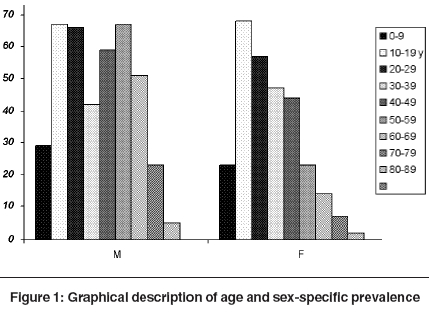
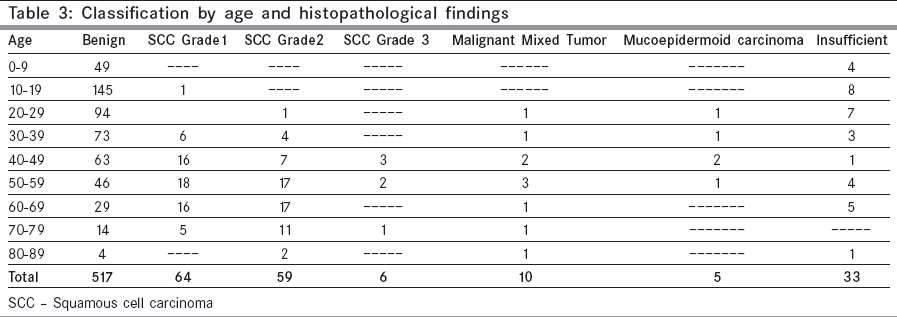
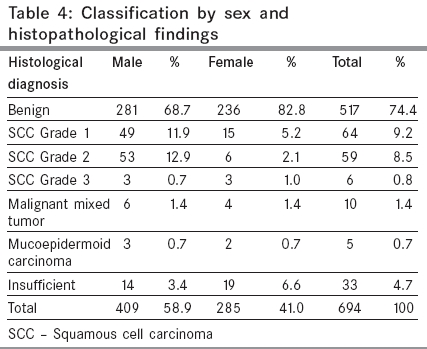
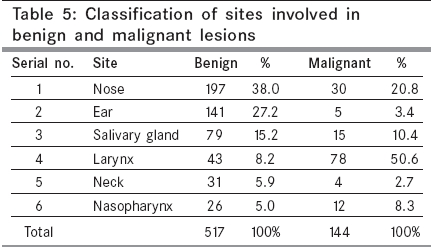
Indian Journal of Cancer, Vol. 42, No. 2, April-June, 2005, pp. 89-93 Original Article Trends of prevalence and pathological spectrum of head and neck cancers in North India Mehrotra Ravi, Singh Mamata, Gupta RajKishore, Singh Manish, Kapoor AnilK Department of Pathology, Moti Lal Nehru Medical College, Allahabad Code Number: cn05017 Abstract BACKGROUND: Head and neck neoplasia constitute one of the commonest cancers in India. Use of smokeless tobacco (Pan masala, Zarda etc.) is on the increase in North India, especially in Uttar Pradesh, and is responsible for the large majority of these tumours.AIM: To assess the patients' characteristics, yearly prevalence and histopathological subtypes of the head and neck neoplasia (excluding oral cavity) in Allahabad and surrounding regions. SETTINGS AND DESIGN: A retrospective study of 11 years from 1990 to 2000 was designed. Data was collected year-wise using the tumor registry data. MATERIAL AND METHODS: All biopsies submitted for histopathology to the Pathology department were reviewed and analyzed for demographic data, site and diagnosis. STATISTICAL ANALYSIS: The Kolmogorov-Smirnov Two-Sample Test was utilized to determine whether two distributions are the same. RESULTS: A total of 40559 biopsies were examined in the department, of which, lesions of the head and neck region, excluding the oral cavity, constituted 694 biopsies (409 males and 285 females). One hundred and forty-four malignant lesions were reported, 114 being males and 30 females. A comparison of the age-specific prevalence rates of cancer during the study period showed that the prevalence was highest in patients belonging to the 50-59 years age group and squamous cell carcinoma Grade II was the most prevalent type. On an average, 58 new biopsies per annum were received. CONCLUSIONS: Properly structured site-specific data like this can augment the National Cancer Registry Programme and is an essential indicator for the magnitude and the pattern of the cancer problem in India. Keywords: Head-neck malignancies, Prevalence, North India, Histopathology Introduction Head and neck neoplasia (HNN) is a major form of cancer in India, accounting for 23% of all cancer in males and 6% in females.[1] The five-year survival varies from 20-90% depending upon the sub-site of origin and the clinical extent of disease. The majority of these neoplasia are preventable. Tobacco and alcohol play an important role in the etio-pathogenesis of HNN. The per capita consumption of cigarettes has increased by 2% over the last decade in the country. Estimates of the number of persons developing the disease annually attributable to tobacco in the mid-eighties included 1,08,000 annual incident biopsies of cancer.[2] India has the dubious distinction of having the world′s highest reported incidence of HNN in women.[3] The disproportionately higher prevalence of HNN in relation to other malignancies in India may be due to the use of tobacco in various forms, consumption of alcohol and low socioeconomic condition related to poor hygiene, poor diet or infections of viral origin.[4] The risk increases in proportion to the intensity and duration of the exposure to each carcinogen. Yet, individual susceptibilities to these risk factors vary within the general population. The basis for this susceptibility may be inborn or acquired, which is still under investigation. The spectrum of HNN varies from place to place within the country. Site-specific data from different parts of the country provide the various trends and give clues to the etiological factors responsible for this significant variation.Materials and Methods A retrospective study of 11 years from 1990 to 2000 was designed. The catchment area of this study was in and around Allahabad. Data was collected year-wise with context to age, sex, site involved and histopathological findings. Records were maintained in the departmental patient registry and were retrieved manually. Various malignancies of the head-neck region were classified according to the International Classification of disease coding system devised by WHO (9th revision) using ICD codes from 140 to 202. The total number of biopsies performed in the hospital formed the basis of all further analysis. This number was used as population (denominator) for further calculation. The departmental ethics committee cleared the study. Statistical analysis was done by utilizing the Kolmogorov-Smirnov two-sample test, which is a non-parametric statistical test.Result A total of 40559 biopsies were received in the Department of Pathology during 1990-2000, of which 694 biopsies (409 were males, 285 were females) were from the head and neck region, except the oral cavity [Table - 1]. Year-wise trends of prevalence revealed a maximum prevalence rate of HNN biopsies of 6 per 1000 biopsies examined in 1999, followed by 5.20 per 1000 during 1996. [Table - 2] depicts the distribution of all head and neck biopsies analyzed by age and sex. A maximum of 135 (19.4%) biopsies were reported in the 10-19 years age group. This probably reflects a high prevalence of these lesions in our region as well as a high index of suspicion. Secondly, parents of children and young adults seek more prompt medical attention than older patients. There were 409 (58.9%) males as compared to 285 (41.1%) females, yielding a male to female ratio of 1.43:1 [Figure - 1]. Of these 694 biopsies, 144 malignant lesions, including 114 males and 30 females, were observed, with a male to female ratio of 3.8:1. This difference in prevalence among males and females was found to be statistically significant (P < 0.05). On an average, 58 new HNN biopsies were received per annum. Examination of biopsies from HNN revealed 517 (74.5%) benign biopsies and 144 (20.7%) malignant lesions, while 33 (4.7%) biopsies remained inconclusive [Table - 3]. The majority of the benign biopsies were reported in the age group of 10-19 years followed by the age group 20-29, whereas the maximum (8 biopsies, 24.2%) in the inconclusive category were in the 10-19 years age group. The majority of the malignant lesions were observed in the 50-59 years age group. Distribution of histological findings among males and females [Table - 4] was found to be statistically significant (P < 0.05) as revealed by the Kolmogrov-Smirnov two-sample test. Among males, squamous cell carcinoma (SCC) of Grade II was more prevalent (13.0%) while among females, squamous cell carcinoma Grade I was more prevalent (5.3%). [Table - 5] depicts the larynx as the most common site involved - observed in 78 patients (54.2%) followed by the nasal cavity in 30 (28.8%). In the benign lesions the nose was the most common site followed by the ear. Discussion Head and neck malignancies (ICD-9 categories 140-149 and 161) are common in several regions of the world where tobacco use and alcohol consumption is high. The age standardized incidence rate of HNN in males exceeds 30/100,000 in regions of France, Hong Kong, the Indian subcontinent, Central and Eastern Europe, Spain, Italy, Brazil, and among the US blacks. High rates (> 10/100,000) in females are found in the Indian subcontinent, Hong Kong and Philippines. The variation in the incidence of cancers by sub-site of head and neck is mostly related to the relative distribution of major risk factors such as tobacco or betel quid chewing, cigarette or bidi smoking, and alcohol consumption. While mouth and tongue cancers are more common in the Indian sub-continent, nasopharyngeal cancer is more common in Hong Kong and pharyngeal and/or laryngeal cancers are more common in other populations. While the overall incidence rates show a declining trend in both sexes in India, Hong Kong, Brazil and US whites, an increasing trend is observed in most other populations, particularly in Central and Eastern Europe, Scandinavia, Canada, Japan and Australia.[5] Allahabad is a central eastern district of Uttar Pradesh with Pratapgarh, Fatehpur and Jaunpur in its North, Varanasi and Mirzapur in the East, Rewa (MP) in South and Banda in the West. Patients from these neighboring regions also approach this institute for treatment. The genesis of these cancers is thought to be closely linked to the use of tobacco and alcohol. Year-wise trends of prevalence revealed a maximum rate of HNN biopsies of 6 per 1000 biopsies examined in 1999 followed by 5.2 per 1000 during 1996. Similar trends for oral cavity cancer had been reported previously by our group.[4] In our study group, we found that the larynx was the most common site observed in 78 patients, 99% of these biopsies had squamous cell carcinoma. The second most common site was the nose observed in 30 patients. On the other hand, Manjari et al reporting on 1471 biopsies of carcinoma of the oral cavity, pharynx, larynx, and the nasal cavity from Amritsar over 10 years, found that the oral cavity was involved in 35.75 % of biopsies and the least prevalent was cancer of the nasal cavity. The males outnumbered females with a male to female ratio of 2.14:1. The maximum prevalence was seen in the fourth and fifth decade. On histopathological examination, 88.2 % biopsies were epidermoid carcinoma followed by anaplastic carcinoma and there was a single case each of mucoepidermoid carcinoma and fibrosarcoma.[6] In our patients, keratinizing and non-keratinizing squamous cell carcinomas of varying grades were found. Several possible predisposing factors have been postulated including race, diet, and occupation etc.[6],[7] Previous radiation alone has been shown convincingly to have a significant influence.[8] These etiologic factors have been recently reviewed by this group.[9] Interpretation of data from a single institution has its clear limitations. The data reflects our specific patient population reporting to the hospital and not the community as a whole. There is an urgent need for an appropriate education program to revert the present trend of preventable head and neck cancers. In a recent report from the Bombay Cancer Registry, Sunny et al found a statistically significant decreasing trend in the overall age-adjusted incidence rates in males during the period 1986 to 2000, with a yearly decrease of 1.7%. This decrease was significant for men above the age of 40, but for young adult men below the age of 40, there was no significant decrease, the level being stable. In females, the overall decreasing trend in the age-adjusted incidence rates of oral cancers was not significant, but in the 40-59 age group, a significant decline was observed.[10] They attributed these findings to a decrease in the usage of pan and tobacco in their target population. We hope to achieve the same results in our population by education and early diagnosis of precancerous and cancerous lesions. Our study was limited by the fact that it was a retrospective survey and the specific histological subtype could not be correlated with dietary habits and other risk factors. A prospective study is planned incorporating the dietary and clinical findings. A multi-institutional study may also help in mapping information regarding the prevalence of this malignancy and aid in allocating necessary resources. While primary prevention is the potential strategy for long-term disease control, early detection and treatment may have limited potential to improve mortality in the short term. Properly structured site-specific data like this can augment the National Cancer Registry Programme (NCRP) and is an essential indicator for the magnitude and the pattern of the cancer problem in India. References
Copyright 2005 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn05017t4.jpg] [cn05017t1.jpg] [cn05017t2.jpg] [cn05017f1.jpg] [cn05017t3.jpg] [cn05017t5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}