 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
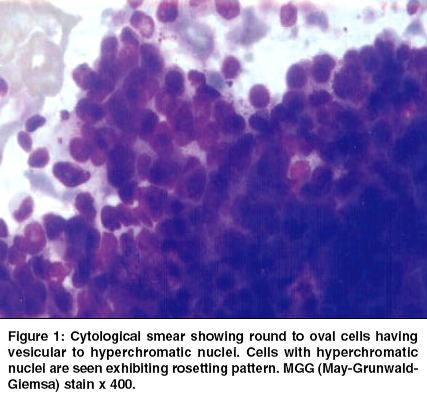
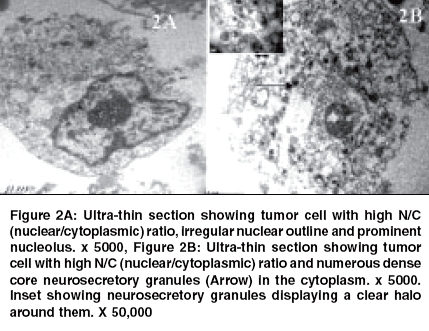
Indian Journal of Cancer, Vol. 42, No. 2, April-June, 2005, pp. 99-101 Case Reports Gastric outlet obstruction and cutaneous metastasis in adenocarcinoid tumor of stomach - Unusual presentations with cytologic and ultra structural findings Rekhi Bharat, Chintamani, Saxena Sunita Institute of Pathology, ICMR and Safdarjung Hospital, New Delhi Code Number: cn05019 Abstract Neuroendocrine tumors, including carcinoids account for less than 1% of gastric tumors. Various subtypes of gastric carcinoids have been reported earlier. The present case deals with two unusual presentations, diagnosis and course of a gastric neuroendocrine tumor in an adult patient. A 35-years-old male initially presented with gastric outlet obstruction for an antral growth in the emergency ward. He underwent radical gastrectomy and was diagnosed with a gastric carcinoid tumor, on histopathology. After 6 months, he developed hepatic along with nodular cutaneous lesions over the scalp. Aspiration cytology (FNAC) from these metastatic lesions showed two distinct cell types with rosette formation. Ultrastructural findings showed neurosecretory granules in some cells. Subsequently, he underwent 2 cycles of chemotherapy. After a total duration of 9 months, he finally succumbed to the disease. We present a case of a gastric adenocarcinoid tumor, with 2 rare presentations. The metastatic lesions exhibited neuroendocrine features on cytology and electron microscopy. Keywords: Gastric adenocarcinoid tumor, Cutaneous metastasis, Ultrastuctural findings, Neuroendocrine tumor Introduction Among the various neuroendocrine tumors (NETs) in the gastrointestinal tract, the small intestine is the commonest site of occurrence and carcinoid tumor is the common pathological type.[1] Gastric carcinoids represent 11-41% of all gastrointestinal endocrine tumors. Lately, an increase in the diagnosis of gastric carcinoids is being seen in western countries, as well as in India. Among the various clinicopathological subtypes, Type I carcinoids are small benign tumors and associated with chronic atrophic gastritis. Type II can be large and polypoid, arise in patients with multiple endocrine neoplasia (MEN-1) and Zollinger-Ellison syndrome. Type III are larger, sporadic, solitary tumors prone to metastasis.[2],[3] On immunohistochemistry aided with tumor markers like NSE (neuron specific enolase), synaptophysin and others, NETs have been categorized into various types i.e. well differentiated carcinoid tumor, malignant carcinoid, small cell carcinoma having an aggressive course, mixed exocrine-endocrine carcinomas and tumor-like conditions.[4] There have been earlier reports on composite (adenocarcinoid) tumors of the gastrointestinal tract.[5] The present case focuses upon two rare presentations of a gastric neuroendocrine tumor. A simple diagnostic technique like FNAC, along with ultrastructural analysis from the metastatic lesions helped in forming an exact diagnosis of an adenocarcinoid tumor in this case.Case History A 35-year-old feeble male presented initially with gastric outlet obstruction in the surgical emergency wing of Safdarjang hospital and was managed by radical gastrectomy. Gross examination revealed a 10 x 6 x 4 cm sized solitary, ulcero- proliferative antral growth. Biopsy showed a tumor beneath gastric mucosa and extending into the muscularis propria, with cells arranged in groups, nests and traberculae. The cells had scanty to moderate amount of cytoplasm and vesicular to hyperchromatic nuclei, revealing prominent nucleolisation in some cells. The tumor was seen reaching up to the pyloric-resected end. Sections from the lymph nodes at Stations I and II revealed tumor deposits. Immunohistochemical staining for CLA (common leukocyte antigen) and CEA (carcino embryogenic antigen) revealed negativity, whereas positive staining was observed with S-100 and NSE (neuron specific enolase). A diagnosis of carcinoid tumor was formed. The postoperative period was uneventful. The patient was discharged on the 10th postoperative day. He remained well until 6 months, when he presented with icterus, tender hepatomegaly and two firm, painless, somewhat nodular cutaneous swellings, one of which measured 5 x 4 cm, extending from the temporal region up to the preauricular sulcus and the other measuring 1.5 x 1 cm over the frontal region of the scalp. There were no symptoms related to carcinoid syndrome. FNAC smears from both the swellings, as well as from the liver (CT-guided) revealed moderate cellularity, comprising two cell types with round to oval tumor cells [Figure - 1]. Whereas some cells showed ducto-acinar arrangements, high N/C (nuclear/ cytoplasmic) ratios, vesicular nuclei having prominent nucleolisation; the others with "salt and pepper" like nuclear chromatin, were arranged in clusters, cords; in rosetting pattern, as well as singly. Cells had a moderate amount of eosinophilic, granular cytoplasm against a background of tumor diathesis. A diagnosis of carcinoma with neuroendocrine differentiation was presumed. A portion of the aspirate was submitted for electron microscopic analysis, which also revealed two types of tumor cells [Figure - 2]. While some tumor cells revealed high N/C (nuclear/cytoplasmic) ratio, irregular, thickened nuclear membranes along with prominent nucleolisation, other tumor cells showed several dense core neurosecretory granules with an outer clear halo effect, in the cytoplasm. The patient was also analyzed for 5HIAA levels (5 hydroxy indole acetic acid), but showed no increase in the levels. There were no symptoms related to carcinoid syndrome. A diagnosis of metastatic adenocarcinoid was finally offered. Following this, he underwent two cycles of chemotherapy. After a total period of 9 months, including both the presentations, he finally succumbed to the disease. Discussion The present case report reveals two unusual presentations, along with the application of FNAC and ultrastructural analysis, for diagnosing a gastric adenocarcinoid tumor. Various types of gastric carcinoids have distinct clinical outcomes and treatment modalities. Type I are generally treated conservatively with endoscopic surveillance and local treatment for tumors less than 1 cm in size and partial gastrectomy for lesions greater than 1 cm. Type II represent 5-10% of gastric carcinoids, are usually multicentric, variably sized and prone to develop lymph node metastasis. They have typical CT (computer tomography) scan findings, with multiple masses in the setting of diffuse gastric wall thickening. Treatment modalities include total gastrectomy, tumor resection, endoscopic polypectomy, instillation of somatostatin analogues.[2], [6] Type III carcinoids, which are likely to be associated with distant metastases and poor survival rates, are treated with chemotherapy, or antitumoral therapies.[3], [6] Thus, typing of these tumors is significant. With the advent of endoscopy, double contrast CT and serum studies of somatostatin, subtyping of these tumors can be made substantially. The possibility of polyps in cases of atrophic gastritis is a strong clinical hint for Type 1 carcinoids.[7] However, in unusual situations of emergency, like gastric outlet obstruction, as in the present case, a diagnosis of carcinoid could be offered on biopsy, supplemented with immunohistochemistry. The following presentation of the patient, with metastatic lesions, prompted a FNAC, which was compounded with electron microscopic analysis to form an exact diagnosis of adenocarcinoid. Adenocarcinoid tumors of the bronchial tree have been described on cytology.[8] Gastric adenocarcinoids are believed to have an aggressive course, over pure carcinoids.[5] Such patients generally present with upper abdominal pain, may be associated with gastrointestinal bleeding and metastatic nodules in the liver. Cutaneous metastasis has also been reported in carcinoids, as in a case by Rodriquez et al,[9] who observed painful cutaneous nodules corresponding to metastasis in a gastric carcinoid tumor, which were confirmed on immunohistochemistry and electron microscopic findings. Another clinical presentation of carcinoid tumors is carcinoid syndrome. A negative history of carcinoid syndrome in this case with non-significant elevation of 5 HIAA (5 hydroxy-indole-acetic acid), was unusual. Expression of neuroendocrine cell differentiation by some cells might have been a cause for the non-expression of symptoms related to carcinoid syndrome. A histopathological diagnosis of adenocarcinoid tumor in the present case was made by excluding the various differential diagnoses, which were mainly constituted by the other NETs, including carcinoids. Ultrastructural findings led to an exact diagnosis of this tumor that was reported as carcinoid tumor on biopsy. This varied pattern of tumor development from carcinoid to adenocarcinoid, in the present case, especially with clinically visible metastatic lesions, explains the aggressive course of this tumor. In short, a range of clinical presentations, along with histopathological subtypes exists for gastric neuroendocrine neoplasms. Electron microscopy on aspirate samples is useful in exact categorization, required for appropriate treatment. References
Copyright 2005 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn05019f2.jpg] [cn05019f1.jpg] |
| |||||||||

{kind=link}
{kind=link}