
|
Indian Journal of Cancer
Medknow Publications on behalf of Indian Cancer Society
ISSN: 0019-509X EISSN: 1998-4774
Vol. 42, Num. 3, 2005, pp. 125-132
|
Indian Journal of Cancer, Vol. 42, No. 3, July-September, 2005, pp. 125-132
Review Articles
Quality of life measures in lung cancer
Anant Mohan, Guleria Randeep, Pathak AshutoshK, Bhutani Manisha, Pal Hemraj, Charu Mohan, Kochupillai V
Departments of Medicine All India Institute of Medical Sciences, Ansari Nagar, New Delhi-110029
Correspondence Address: Dr Randeep Guleria, E-mail: randeepguleria2002@yahoomail.com
Code Number: cn05022
Abstract Lung cancer is one of the leading causes of cancer death worldwide. Survival has not improved significantly in spite of newer therapies. In view of the high-symptom burden and severe morbidity, evaluation of quality of life (QOL) becomes important in these patients. Several instruments are now available for this purpose, and have demonstrated good correlation with performance status, symptoms, and survival. Quality of life assessments also help in comparing different therapeutic regimes, thus allowing selection of the appropriate modality. Problems of inconsistent interpretability and high-patient dropout rate poses a challenging problem that needs to be tackled. In spite of these drawbacks, QOL is now considered to be an essential component of lung cancer management and should be performed routinely. Such a practice will help the physician plan appropriate treatment strategies and set practical therapeutic goals.
Keywords: Lung cancer, Performance status, Quality of life
Introduction
Lung cancer is one of the leading causes of cancer deaths globally. It carries a greater mortality than colorectal, breast and prostate cancers collectively. In the year 2000 alone, lung cancer was responsible for 692 000 male and 156 000 female deaths.[1] Approximately
85% of patients with lung cancer are diagnosed at an advanced stage that is not amenable to surgical intervention. As a result, these patients require chemotherapy and/or radiotherapy. In spite of several advancements in the chemotherapeutic regimens and the addition of many newer drugs, the 5-year survival has improved only marginally from 5% in the 1950s to approximately 14% by
1996.[2] The overall 1-year
survival is less than 20%. Moreover, lung cancer is not just associated
with a high mortality but a high morbidity as well, with a significant
proportion of patients severely incapacitated by disease-related symptoms
such as chest pain, cough, hemoptysis, and dyspnea.[3] In such a grim scenario, the evaluation and improvement of quality of life (QOL) as well as alleviation of symptom distress assumes great importance in the overall management of these patients.
Definition of quality of life
The assessment of a patient of cancer broadly includes two sets of
endpoints - cancer outcomes and patient outcomes. Cancer outcomes measure
the response of a patient to treatment, duration of response, symptom
free period, and early recognition of relapse. Patient outcomes, on the
other hand, assess the survival benefit attained after treatment as measured
by the increase in life span, and the QOL before and after therapy. Unfortunately,
physicians tend to concentrate on the cancer-related outcomes only. Consequently,
assessment of QOL remains a neglected area.
Quality of life is a broad, subjective, and multidimensional concept
that includes:
- Physical health and symptoms.
- Functional status and activities of daily living.
Mental well being and social health, including social role functioning.
Quality of life can also be simply defined as the effect of an illness
and its therapy upon a patient′s physical, psychological, and
social well being as perceived by the patient himself.[4] However,
being a highly subjective variable, there can be no universal consensus
over this definition. The intra- and inter-observer variation can be
large, and more importantly, may even vary at different points of time.
Since it is impossible to define any universally agreed standard for
comparison, the subject and observer usually have different perceptions
of the same outcome. Furthermore, significant subjective variability
may exist within the same patient regarding his problems. For example,
he may endure pain for a short while without compromising his daily
activities, but over an extended period, this pain may dominate his
life and cause
significant impairment of various activities.
Over the past few years, increasing attention is being paid to the
evaluation of QOL in various diseases, including lung cancer. Numerous
instruments
have been developed, mainly in the form of questionnaires, which were
subsequently validated in different settings and translated in several
languages. However, other techniques, such as personal or telephone
interviews, may also be used for this purpose. Measuring QOL is especially
useful
in phase-III trials since it allows the investigator to make, in most
cases, definite conclusions regarding the efficacy of a particular
therapeutic regimen. Quality of life assessments should be given due
priority whenever
it is expected that the survival differences between the treatment
groups is going to be small (a frequent occurrence), or when the difference
in at least one factor predicting QOL is expected to be large. The
effect
of two different therapeutic modalities on QOL and overall survival
helps select the better modality. In fact, a particular treatment may
be preferred
if it improves the QOL even if the survival is not superior to the
other. On the other hand, a treatment may be unsatisfactory and may
be rejected
if the QOL remains similar or worsens compared to another modality,
without offering any survival advantage. However, two situations present
a difficulty:
one, if the treatment improves QOL but worsens survival, and, when
QOL deteriorates but survival improves. In these situations, the choice
of
treatment is usually made jointly by the physician and the patient
after detailed consideration of all relevant aspects.
Attributes of an ideal quality of life instrument[5]
Any QOL questionnaire should possess the following attributes:
- Reproducibility: ability to yield the same results repeatedly
under the same conditions.
- Validity: accuracy with which it measures what it is supposed to
measure.
- Responsiveness: ability to detect clinically significant changes
over time.
- Interpretability: ability to provide results that can make sense.
Quality of life and lung cancer
Quality of life is closely linked to symptom burden and severity
in lung cancer. Loss of physical functioning, psychological events
such as depression, and reduced overall QOL is associated with uncontrolled
symptoms.[6],[7] In
addition, depression has also been found to be an independent prognostic
factor for lung cancer irrespective of stage.[8]
Physical functioning is possibly the easiest to evaluate in QOL studies.
However, they have their own limitations. The commonest symptoms
of lung cancer, i.e. cough, and dyspnea may be caused by chronic
bronchitis
also,
whereas hemoptysis is usually transient. It has been suggested that
pain and malaise are the most useful symptoms for assessing general
well being
in lung cancer. Likewise, nausea, vomiting, and hair loss are proposed
to be the most suitable symptoms for evaluating treatment-related
side effects.[9]
It is now universally accepted that assessment of QOL should be included
in evaluating treatment outcomes in lung cancer. A recent review,
that examined all prospective phase III randomized trials for the
treatment
of lung cancer found that only 14 out of 39 studies (36%)
contained information about QOL.[10] Only
five of these used QOL and symptom relief as primary end-points;
majority of the remaining described patient-reported symptom assessment.
A previous
review that examined 151 QOL studies in lung cancer found that 83
focused specifically on either small cell cancer or nonsmall-cell
lung cancer.[11] Of
these 151 reports, 33 were validation/feasibility studies. The remaining
studies were carried out with different objectives, using varying
time intervals of measurement, different clinical outcomes, and different
interpretations of QOL changes.
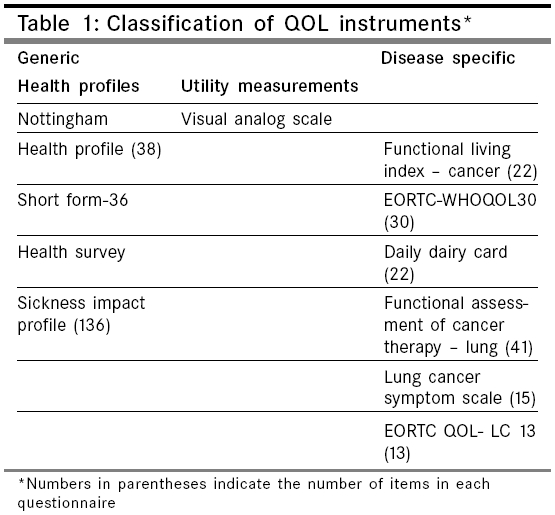
Over the last decade, over 50 instruments have been developed and
used to measure QOL in lung cancer. Quality of life instruments are
mainly
classified in the following categories: generic or disease-specific.
Generic instruments are further subclassified into Health profiles
and Utility measurements [Table - 1].
Health profiles are single instruments primarily used to measure
each important facet of QOL. They have the advantage of being valid
and
reproducible over a wide variety of diseases, as well as being able
to demonstrate
change with treatment. However, they are not disease-specific and
hence, may miss important aspects of QOL of the disease under evaluation.
They are also lengthy and time-consuming compared to the recent site-specific
questionnaires available.
Utility measurements, on the other hand, measure an individual′s
perception of a single symptom, e.g. dyspnea or chest pain. The commonest
in use is the Visual analog scale (VAS). This is a vertical line
10 cm in length with two anchor points at each extreme. The two ends
may be
designated verbal descriptions such as none and maximum. The subject
responds by marking a point on the line to indicate the intensity
of the symptom as perceived by him. Visual analog scale eliminates
the restrictions
imposed by fixed responses (better/worse, or yes/no), and allows
a flexible response in a continuum, thereby allowing finer descriptions
and assessments
of any subjective state. Visual analog scale has been extensively
used in QOL studies, mostly to quantify dyspnea, and has been found
to be
a reliable and reproducible tool.[12],[13]
Disease-specific questionnaires are those that incorporate questions
relevant to a particular disease. These may include items pertaining
to symptoms and treatment-related toxicities. The commonly used specific
QOL instruments for lung cancer are the Functional Assessment of
Cancer Therapy-Lung (FACT-L), Lung Cancer Symptom Scale (LCSS), and
the European
Organization for Research and Treatment of Cancer Quality of Life
Questionnaire-Lung Cancer (EORTC-QLQ-LC 13).
Most of the instruments listed in [Table
- 1] have
been widely applied in QOL assessment studies. However, there is
a substantial heterogeneity in the outcome variable(s) used to evaluate
QOL. Some questionnaires
use changes in symptom burden and severity as the indicator of QOL,
whereas others use subscale scores to measure change over time and
with intervention.
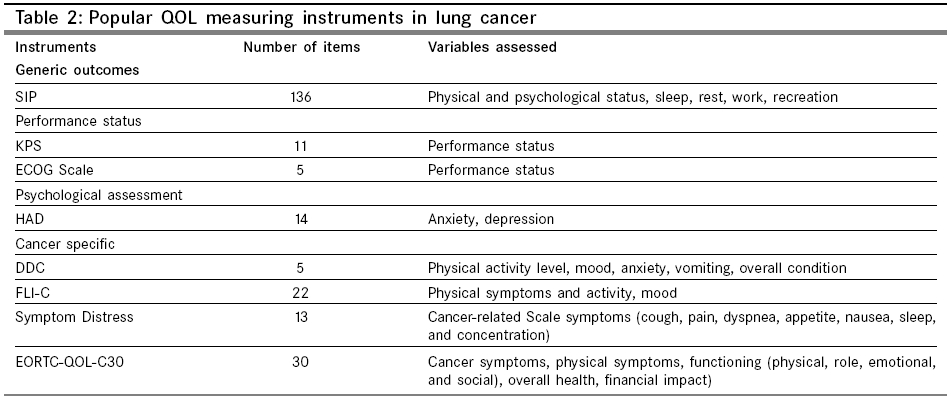
Some of the popular instruments, categorized according to the primary
outcome measured, are shown in [Table
- 2].
These instruments are useful not only for baseline evaluation, but
also to assess the efficacy of various therapeutic modalities (including
surgery,
chemotherapy, and radiotherapy) or a combination of any of the above.
The description of how a particular treatment (or combination of
treatments) influences the QOL and overall survival is important
to assist in the
selection of the best possible approach.[14] This
has important implications for the patient who may, in fact, opt
for the treatment that offers a better QOL even if the overall survival
is not superior to that conferred by another treatment regimen.[4]
Among the instruments listed in [Table
- 1] , the
FACT-L, the European Organization for Research and Treatment of Cancer
Quality-of-Life Questionnaire (EORTC QLQ C30) (along with its lung
cancer specific module), and LCSS are the most widely used for QOL
assessments
in lung cancer clinical trials.
Functional assessment of cancer therapy-lung
The
FACT instrument
was developed
to measure
QOL in
patients with cancer.[15] The
original questionnaire, referred to as the FACT-General (FACT-G),
comprised
of 27 items. The lung cancer-specific module (FACT-L) incorporates
the FACT-G
with a symptom scale specific for lung cancer. The latest version
(Version 4) is a 41-item self-reported questionnaire. Among
these, 34 items
pertain to five dimensions of general health-related QOL (physical,
social and
family, emotional, functional well-being, and relationship with the
physician), and seven items to specific lung cancer symptoms (dyspnea,
difficulty
breathing, coughing, chest tightness, appetite, weight loss, and
cognitive function). These items are marked on a 5-point
Likert scale keeping
a time frame of the past 1 week. This questionnaire has the disadvantage
of putting less emphasis on treated related symptoms. However, in
spite of these shortcomings, it has a high level of reliability
and validity
based on extensive psychometric testing.[16] Good
sensitivity to change has also been demonstrated. A change of two
points on the seven-item symptom scale is considered a clinically
significant
change in QOL.[17]
European organization for the treatment and research of cancer quality of life questionnaire (EORTC QLQ-C30) and EORTC QLQ LC 13
In order to overcome
the shortcomings of
the QOL instruments
existing at the
time, the EORTC initiated
a large-scale multinational
program
in 1986 to try and develop a comprehensive questionnaire that covers
all areas of QOL assessment. This program included 305 patients across
13 countries. The outcome was a 30-item questionnaire, which included
five functional scales (physical, role, cognitive, emotional, and
social), three symptom scales (fatigue, pain, nausea, and
vomiting), and one
global health and QOL scales. This instrument was tested in the USA,
Australia,
Europe, and Japan and demonstrated a high reliability and validity
across the continents.[18]
The EORTC QLQ-LC 13 questionnaire was developed in 1994 as a lung
cancer specific supplementary to the EORTC QLQ-C30. This is a 13-item
instrument
that assesses lung cancer related symptoms [cough and hemoptysis
(one item each), dyspnea (three items)], treatment related side-effects
[sore mouth or tongue, dysphagia, hair loss, tingling hands, and
feet
(one
item each)], pain (three items), and pain medication (one item).
All items are rated on a 4-point Likert scale and 7-point numerical
analog
scale with a reporting time frame of 1 week. Extensive field studies
demonstrated significant changes in symptom and treatment toxicity
subscale scores over time, with symptoms improving and treatment
related side
effects increasing during chemotherapy.[19] Thus,
it was found to be a clinically valid and useful tool to assess disease
and treatment-specific symptoms in lung cancer patients. The EORTC-QLQ
C30 and EORTC-QLQ LC-13 are often used together in order to obtain
a comprehensive evaluation of QOL in lung cancer. Over the last decade,
it has been translated into 17 other languages and is now the most
widely
used QOL questionnaire in cancer patients.
Methods of analysis of this questionnaire and interpretation of clinically
meaningful changes of QOL measures have varied. Some studies calculated
changes in individual symptom scores whereas others used mean subscale
scores of the various QOL domains to evaluate change. [20],[21],[22] Montazeri
et al. compared EORTC scores in 129 patients divided into two groups,
one who received treatment (chemotherapy, radiotherapy, or surgery)
and the other that did not (called as receiving best supportive care).[23] They
used the change in mean scores of individual symptoms as well as
mean subscale domain scores to interpret the results. Some researchers
categorized
symptom changes into subgroups, such as improved, worsened, or unchanged.[24]
Lung cancer symptom scale
This
questionnaire
was developed in the mid-1980s
at the Memorial Sloan-Kettering
Cancer
Center as a
lung cancer-specific
questionnaire
that focuses primarily on the physical and functional dimensions
of a patient. It comprises two different scales, one rated
by the patient
and the other by the physician. The patient scale contains nine items,
including three summation and six symptom items. Each item is marked
on a VAS of 100 mm length, with zero denoting the lowest rating and
100
the highest. The mean of the six main symptoms is used to calculate
the ′average symptom burden′of
the patient. The physician scale consists of six items pertaining
to the main lung cancer symptoms. These are rated as 0, 25, 50, 75,
and
100 depending on symptom severity.[25]
A change of 10 mm or more on the patient scale is taken as a clinically
meaningful change in QOL and has been found to correlate well with
symptomatic change both for total score and for individual items.[26] A
drawback of LCSS is that it ignores several important components
of QOL, such as the social and emotional aspects. However, Hollen
and
Gralla
compared LCSS with other QOL instruments and demonstrated a reasonably
good reliability and validity.[27] Normative
data is also available in a large cohort of NSCLC patients.[28] Consequently,
LCSS remains popular and has been used in several studies for assessing
QOL.[29],[30]
Problems in measuring quality of life
Measuring
QOL is
beset with
several
problems. There
is a large intra and inter-observer
error, and perceptions
may vary with time.
There is
no universal agreement regarding comparative standards. Except for
the Nottingham Health Profile (NHP), which was developed through
public participation,
majority of questionnaires were devised by physicians.[31] As
a result, subjective variability is high since different physicians
may have different points of view. Barriers of language, culture,
and religion
also hinder accurate measurement of QOL. In addition, several other
factors such as age, associated co-morbidities, and the quality of
medical and
palliative care provided to the patients influence many aspects of
QOL. Comparing two studies is difficult since they invariably differ
in the
patient profile, timings of assessments, treatment modalities given,
length of follow-up, and the QOL instrument used for evaluation.
Furthermore, the short-term survival of lung cancer, rapid deterioration
of performance
status (PS), and drop-outs due to treatment related side effects
may cause difficulty in collecting data and following-up the patients
for
a long period of time. This problem of ′missing data′ causes difficulties in making accurate assessments and drawing conclusions from QOL studies. It has been suggested that comparative analysis of QOL should be stopped when less than 30% of
the data is available.[32]
Performance status and quality of life
Performance
status
has been
frequently
used as a proxy
of QOL since the 1970s.
It is an important
prognostic factor
and predictor
of survival
of lung cancer patients.[8] There
is good correlation between PS and global QOL, including psychological,
physical, and symptomatic well-being. Performance status also correlates
well with the number and severity of symptoms.[33] The
most well established markers of PS are the Karnofsky Performance
Scale (KPS) and the Eastern Cooperative Oncology Group (ECOG). Karnofsky
Performance Scale is a simple and widely used numerical instrument
for rapidly quantifying
the PS of an individual based on his level of independence.[34] This
scale rates the PS of a patient in multiples of 10, from 0 (worst)
to 100 (best) depending on the ability to perform his activities.
Various studies have demonstrated a direct relationship between KPS
and the
perceived
QOL in patients with cancer, including lung cancer.[8] In
a study of 57 disease free survivors of lung cancer, KPS was found
to be the best predictor of QOL.[35] However,
another study that evaluated 139 patients of lung cancer receiving
palliative treatment, KPS was found to be only weakly associated
with the QOL as
measured by EORTC QLQ C30.[36]
Similar results have been observed in studies that used the ECOG
Scale. This scale is a five-grade observer rating of patients′physical
ability ranging from 0 (normal) to 4 (disabled).[37] Buccheri
and Ferrigno performed a validation study using ECOG and KPS on a
large sample of 471 patients and concluded that both instruments
are valid,
however, the ECOG was found to be slightly superior.[38] Aaronson
et al. used the ECOG and EORTC QLQ-C30 to evaluate QOL in 354 patients
with lung cancer undergoing chemotherapy or radiotherapy.[8] They
found a strong correlation between the PS (assessed by ECOG scale)
and physical, role, cognitive functioning, and overall QOL (assessed
by EORTC
QLQ-C30). These results suggest that measurement of PS by either
KPS or ECOG may serve as a useful and simple surrogate marker of
QOL.
Quality of life as a prognostic marker in lung cancer
There
is sufficient
evidence to suggest
that initial QOL
is a strong
prognostic
factor for survival in lung
cancer. Ganz et
al.
demonstrated
the predictive value of QOL [assessed by Functional Living Index-Cancer
(FLI-C)] for survival in 40 patients receiving either chemotherapy
or radiotherapy.[39] In
another large study, the pretreatment QOL as assessed by the FLI-C
strongly prognosticated
a randomized sample of 437 patients undergoing two different therapeutic
regimens.[40] Langendijk
et al evaluated baseline QOL using EORTC QLQ C30 in 198 patients
planned for radiotherapy and estimated the prognostic value of several
parameters
for survival.[41] Performance
status, weight loss, and N-classification were found to be independent
prognostic factors. Global QOL was the strongest predictor of survival
after multivariate analysis. A 3-month follow-up assessment of QOL
in 129 patients showed that prediagnosis global QOL was the most
significant predictor of the length of survival after adjusting for
other known
prognostic
factors such as age and extent of disease.[23] Other
important proposed prognostic markers are the subscales - pain, anorexia,
fatigue, lung cancer symptoms, level of physical functioning, overall
QOL, albumin, and the stage of disease.[42] There
does not appear to be any significant correlation with histological
subtype.
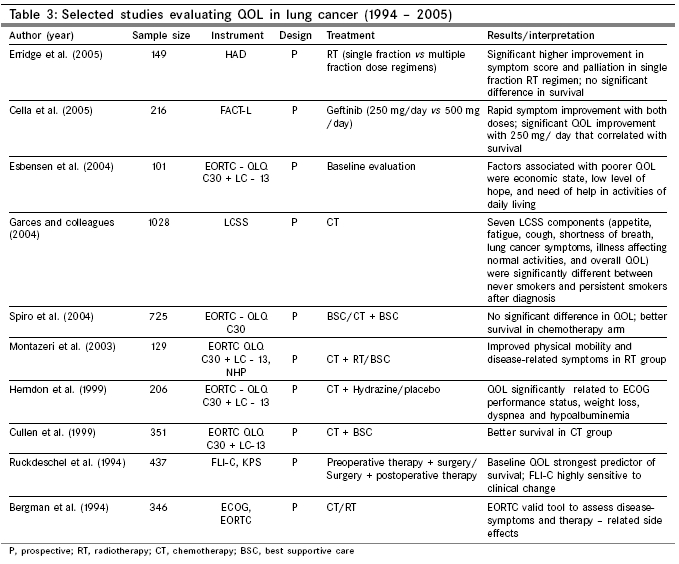
The association of QOL with chemotherapy has been evaluated in several
studies [Table - 3].
Helsing et al compared chemotherapy with best supportive care and
demonstrated significant survival benefit in the chemotherapy group
(29 weeks vs 11
weeks; 1-year survival, 28% vs 8%) along with
significant improvement in dyspnea, pain, insomnia, and social function.[43] Similarly,
the Elderly Lung Cancer Vinorelbine Study Group found significantly
longer survival, less pain and dyspnea, better cognitive function
and QOL, and
better global health status in the vinorelbine group compared to
controls.[44] In
contrast, Bonomi et al. compared two chemotherapeutic regimes (paclitaxel/cisplatin vs etoposide/cisplatin)
and found a significant decline in QOL over time inspire of improved
survival in the paclitaxel/cisplatin arm.[45]
From the above evidence, therefore, it is clear that the benefit
of chemotherapy over best supportive care is still questionable.
A clear
answer to this
question would be difficult since most chemotherapeutic regimes have
produced benefit in different aspects of the disease, such as survival,
symptomatic relief, tumor regression, and QOL.
Conclusion
Lung cancer continues to claim thousands of lives every year globally.
Several newer therapies have, as yet, failed to significantly prolong
survival or offer curative benefit. In view of the high morbidity and
short survival, assessment of QOL needs to be included as an end point
in evaluation and treatment of lung cancer. Several instruments, mostly
in the form of questionnaires, have been developed in the last decade,
and subsequently translated and cross-validated in various geographical
and cultural settings. Quality of life measurements also help in predicting
survival, evaluating efficacy of various treatment regimens, as well
as comparing one regimen with another. However, several problems, such
as missing data due to a high-dropout rate, and lack of guidelines for
uniform interpretation still exist that need to be addressed and improved
upon in the future. In spite of these handicaps, QOL evaluation would
greatly help in treatment planning and in the setting up of appropriate
and practical therapeutic goals. As far as the patient is concerned,
the primary goal of the physician should be to try and improve his overall
QOL using all measures available.
References
| 1. | GLOBOCAN 2000: Cancer incidence, mortality and prevalence worldwide, version 1.0. IARC cancer base No. 5, IARC press: Lyon; 2001. Back to cited text no. 1 |
| 2. | Ries LA, Kosary CL, Hankey BF. Lung and bronchus cancer: SEER Cancer Statistics Review, 1973-1996. National Cancer Institute: Bethesda, MD; 1999. Back to cited text no. 2 |
| 3. | Cooley ME. Symptoms in adults with lung cancer: a systematic research review. J Pain Symptom Manage 2000;19:137-53. Back to cited text no. 3 [PUBMED] [FULLTEXT] |
| 4. | Roila F, Cortesi E. Quality of life as a primary end point in oncology. Ann Oncol 2001;12:3-6. Back to cited text no. 4 [PUBMED] |
| 5. | Fayers PM, Jones DR. Measuring and analyzing quality of life in cancer clinical trials: a review. Stat Med 1983;2:429-46. Back to cited text no. 5 [PUBMED] |
| 6. | Montazeri A, Milroy R, Gillis CR, McEwen J. Quality of life: perception of lung cancer patients. Eur J Cancer 1996;32A:2284-9. Back to cited text no. 6 [PUBMED] |
| 7. | Gridelli C, Perrone F, Nelli F, Ramponi S, De Marinis F. Quality of life in lung cancer patients. Ann Oncol 2001;12:S21-5. Back to cited text no. 7 [PUBMED] |
| 8. | Buccheri G, Ferrigno D. Prognostic factors in lung cancer: tables and comments. Eur Respir J 1994;7:1350-64. Back to cited text no. 8 [PUBMED] |
| 9. | Geddes DM. Quality of life in lung cancer. Respir Med 1991;85:7-11. Back to cited text no. 9 [PUBMED] |
| 10. | Sarna L, Riedinger MS. Assessment of quality of life and symptom improvement in lung cancer clinical trials. Semin Oncol 2004;31:1-10. Back to cited text no. 10 [PUBMED] |
| 11. | Montazeri A, Gillis CR, McEwen J. Quality of life in patients with lung cancer: a review of literature from 1970 to 1995. Chest 1998;113:467-81. Back to cited text no. 11 [PUBMED] [FULLTEXT] |
| 12. | Bond A, Lader M. Use of analog scales in rating subjective feelings. Br J Med Psychol 1974;47:211-8. Back to cited text no. 12 |
| 13. | Gift AG. Validation of a vertical visual analog scale as a measurement of clinical dyspnea. Rehab Nursing 1989;14:323-5. Back to cited text no. 13 [PUBMED] |
| 14. | Feld R. Endpoints in cancer clinical trials: is there a need for measuring quality of life? Support Care Cancer 1995;118:622-9. Back to cited text no. 14 |
| 15. | Cella DF, Tulsky DS. Quality of life in cancer: definition, purpose, and method of measurement. Cancer Invest 1993;11:327-36. Back to cited text no. 15 [PUBMED] |
| 16. | Cella DF, Bonomi AE, Lloyd SR, Tulsky DS, Kaplan E, Bonomi P. Reliability and validity of the functional assessment of cancer therapy-lung (FACT-L) quality of life instrument. Lung Cancer 1995;12:199-220. Back to cited text no. 16 [PUBMED] [FULLTEXT] |
| 17. | Cella D, Eton DT, Fairclough DL, Bonomi P, Heyes AE, Silberman C, et al . What is a clinically meaningful change on the functional assessment of cancer therapy-lung (FACT-L) questionnaire? Results from Eastern Cooperative Oncology group (ECOG) Study 5592. J Clin Epidemiol 2002;55:285-95. Back to cited text no. 17 |
| 18. | Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al . The European Organization for Research and Treatment of Cancer QLQ-C30: a quality of life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 1993;85:365-76. Back to cited text no. 18 |
| 19. | Bergman B, Aaronson NK, Ahmedzai S, Kaasa S, Sullivan M. The EORTC QLQ-LC13: a modular supplement to the EORTC core quality of life questionnaire (QLQ-C30) for use in lung cancer clinical trials. EORTC Study Group on quality of life. Eur J Cancer 1994;30:635-42. Back to cited text no. 19 |
| 20. | Cardenal F, Lopez-Cabrerizo MP, Anton A, Alberola V, Massuti B, Carrato A, et al . Randomized phase III study of gemcitabine-cisplatin versus etoposide-cisplatin in the treatment of locally advanced or metastatic non-small cell lung cancer. J Clin Oncol 1999;17:12-8. Back to cited text no. 20 |
| 21. | Gatzemeier U, von Pawel J, Gottfried M, ten Velde GP, Mattson K, DeMarinis F, et al . Phase III comparative study of high-dose cisplatin versus a combination of paclitaxel and cisplatin in patients with advanced non-small cell lung cancer. J Clin Oncol 2000;18:3390-9. Back to cited text no. 21 |
| 22. | Crino L, Scagliotti GV, Ricci S, De Marinis F, Rinaldi M, Gridelli C, et al . Gemcitabine and cisplatin versus mitomycin, ifosfamide, and cisplatin in advanced non-small cell lung cancer. A randomized phase III study of the Italian lung cancer project. J Clin Oncol 1999;17:3522-30. Back to cited text no. 22 |
| 23. | Montazeri A, Milroy R, Hole D, McEwen J, Gillis CR. Quality of life in lung cancer patients: as an important prognostic factor. Lung Cancer 2001;31:233-40. Back to cited text no. 23 [PUBMED] [FULLTEXT] |
| 24. | Smith IE, O'Brien ME, Talbot DC, Nicolson MC, Mansi JL, Hickish TF, et al . Duration of chemotherapy in advanced non-small cell lung cancer: a randomized trial of three versus six courses of mitomycin, vinblastine, and cisplatin. J Clin Oncol 2001;19:1336-43. Back to cited text no. 24 |
| 25. | Hollen PJ, Gralla RJ, Kris MG, Cox C. Quality of life during clinical trials: conceptual model for the Lung Cancer Symptom Scale (LCSS). Support Care Cancer 1994;2:213-22. Back to cited text no. 25 [PUBMED] |
| 26. | Frasci G, Lorusso V, Panza N, Comella P, Nicolella G, Bianco A, et al . Gemcitabine plus vinorelbine versus vinorelbine alone in elderly patients with advanced non-small cell lung cancer. J Clin Oncol 2000;18:2529-36. Back to cited text no. 26 |
| 27. | Hollen PJ, Gralla RJ. Comparison of instruments for measuring quality of life in patients with lung cancer. Semin Oncol 1996;23:31-40. Back to cited text no. 27 |
| 28. | Hollen PJ, Gralla RJ, Kris MG, Eberly SW, Cox C. Normative data and trends in quality of life from the Lung Cancer Symptom Scale (LCSS). Support Care Cancer 1999;7:140-8. Back to cited text no. 28 [PUBMED] [FULLTEXT] |
| 29. | Klastersky J, Paesmans M. Response to chemotherapy, quality of life benefits and survival in advanced non-small cell lung cancer: review of literature results. Lung Cancer 2001;34:S95-101. Back to cited text no. 29 [PUBMED] [FULLTEXT] |
| 30. | Svobodnik A, Yang P, Novotny PJ, Bass E, Garces YI, Jett JR, et al . Quality of life in 650 lung cancer survivors 6 months to 4 years after diagnosis. Mayo Clin Proc 2004;79:1024-30. Back to cited text no. 30 |
| 31. | McEwen J, Mckenna SP. Nottingham Health Profile. In : Spilker B, editor. Quality of Life and Pharmacoeconomics in clinical trials. 2nd edn. Lippincott-Raven: Philadelphia; 1996. p. 281-6. Back to cited text no. 31 |
| 32. | Ranson M, Davidson N, Nicolson M, Falk S, Carmichael J, Lopez P, et al . Randomized trial of paclitaxel plus supportive care versus supportive care for patients with advanced non-small cell lung cancer. J Natl Cancer Inst 2000;92:1074-80. Back to cited text no. 32 |
| 33. | Hopwood P, Stephens RJ. Symptoms at presentation for treatment in patients with lung cancer: implications for the evaluation of palliative treatment. Br J Cancer 1995;71:633-6. Back to cited text no. 33 [PUBMED] |
| 34. | Karnofsky DA, Burchenal JH. The clinical evaluation of chemotherapeutic agents in cancer. In : MacLeod CM, editors. Evaluation of chemotherapeutic agents. Columbia University Press; New York; 1949. p. 191-205. Back to cited text no. 34 |
| 35. | Schag CA, Ganz PA, Wing DS, Sim MS, Lee JJ. Quality of life in adult survivors of lung, colon, and prostate cancer. Qual Life Res 1994;3:127-41. Back to cited text no. 35 |
| 36. | Schaafsma J, Osoba D. The Karnofsky performance status scales re-examined: a cross-validation with the EORTC-30. Qual Life Res 1994;3:413-24. Back to cited text no. 36 [PUBMED] |
| 37. | Zubrod CG, Scheiderman MA, Frei E. Appraisal of methods for the study of chemotherapy in man: comparative therapeutic trial of nitrogen mustard and triethylene thiophosphoramide. J Chronic Dis 1960;11:7-33. Back to cited text no. 37 |
| 38. | Buccheri GF, Ferrigno D. Karnofsky and ECOG performance status in lung cancer:equivalence, construct validity, and predictive validity (abstract). Lung Cancer 1994;11:S87. Back to cited text no. 38 |
| 39. | Ganz PA, Lee JJ, Siau J. Quality of life assessment: an independent prognostic variable for survival in lung cancer. Cancer 1991;67:3131-5. Back to cited text no. 39 [PUBMED] |
| 40. | Ruckdeschel JC, Piantadosi S. Quality of life in lung cancer surgical adjuvant trials. Chest 1994;106:324-8. Back to cited text no. 40 |
| 41. | Langendijk H, Aaronson NK, de Jong JM, ten Velde GP, Muller MJ, Wouters M. The prognostic impact of quality of life assessed with the EORTC QLQ-C30 in inoperable non-small cell lung carcinoma treated with radiotherapy. Radiother Oncol 2000;55:19-25. Back to cited text no. 41 [PUBMED] [FULLTEXT] |
| 42. | Herndon JE 2nd, Fleishman S, Kornblith AB, Kosty M, Green MR, Holland J. Is quality of life predictive of the survival of patients with advanced non-small cell lung carcinoma? Cancer 1999;85:333-40. Back to cited text no. 42 [PUBMED] [FULLTEXT] |
| 43. | Helsing M, Bergman B, Thaning L, Hero U. Quality of life and survival in patients with advanced non-small cell lung cancer receiving supportive care plus chemotherapy with carboplatin and etoposide or supportive care only. A multicentre randomized phase III trial. Joint Lung Cancer Study Group. Eur J Cancer 1998;34:1036-44. Back to cited text no. 43 [PUBMED] [FULLTEXT] |
| 44. | Effects of vinorelbine on quality of life and survival of elderly patients with advanced non-small-cell lung cancer. The Elderly Lung Cancer Vinorelbine Italian Study Group. J Natl Cancer Inst 1999;91:66-72. Back to cited text no. 44 [PUBMED] [FULLTEXT] |
| 45. | Bonomi P, Kim K, Fairclough D, Cella D, Kugler J, Rowinsky E, et al . Comparison of survival and quality of life in advanced non-small-cell lung cancer patients treated with two dose levels of paclitaxel combined with cisplatin versus etoposide with cisplatin: results of an Eastern Cooperative Oncology Group trial. J Clin Oncol 2000;18:623-31. Back to cited text no. 45 |
Copyright 2005 - Indian Journal of Cancer
The following images related to this document are available:
Photo images
[cn05022t1.jpg]
[cn05022t3.jpg]
[cn05022t2.jpg]
|

{kind=link}
{kind=link}
{kind=link}