 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
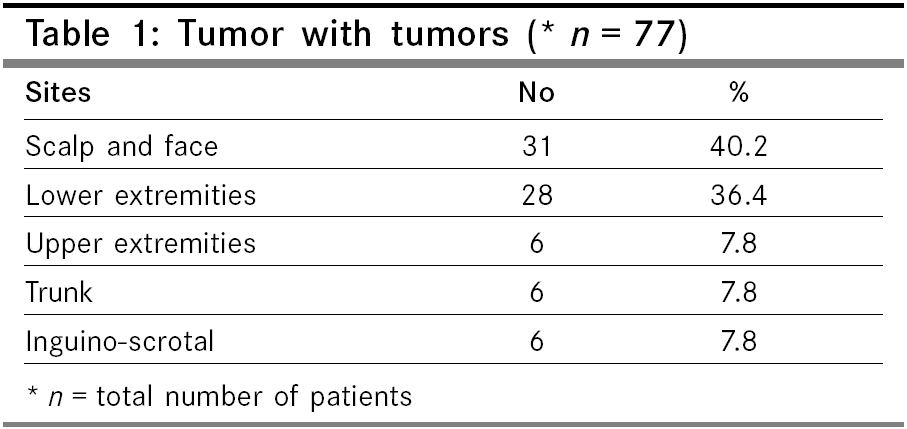
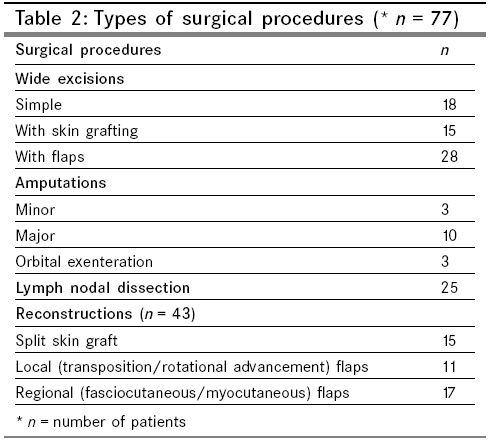
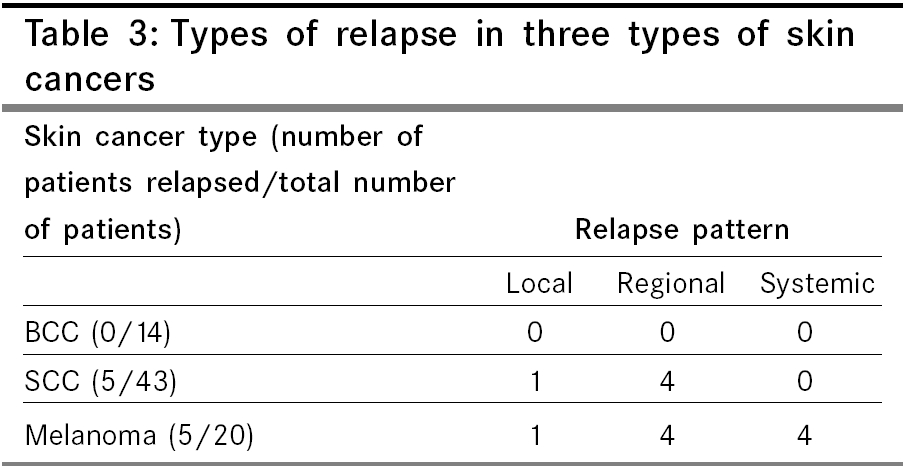
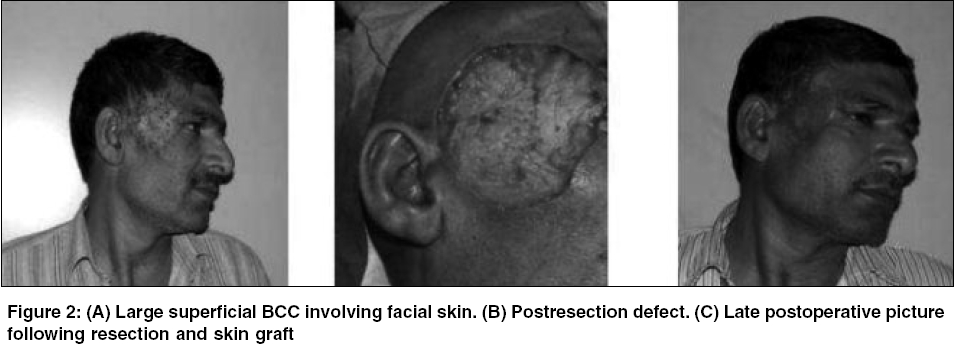
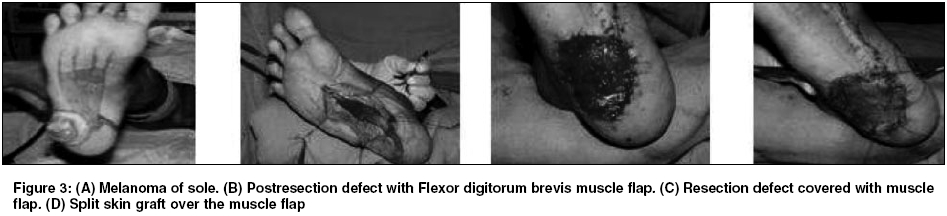
Indian Journal of Cancer, Vol. 42, No. 3, July-September, 2005, pp. 145-150 Original Article Surgical management of skin cancers: Experience from a regional cancer centre in North India Deo SV, Hazarika Sidhartha, Shukla NootanK, Kumar Sunil, Kar Madhabananda, Samaiya Atul Department of Surgical Oncology, Institute Rotary Cancer Hospital, All India Institute of Medical Sciences, New Delhi Code Number: cn05025 Abstract Aims: To review the disease profile and treatment outcome of patients with primary skin malignancies treated at a regional cancer centre. Keywords: Basal cell carcinoma, Malignant melanoma, Reconstruction, Skin cancers, Squamous cell carcinoma, Surgical margins Introduction Skin cancers are relatively uncommon malignancies worldwide, not ranking among the first ten common cancers.[1] There has been a progressive increase in the incidence of skin cancers, particularly that of cutaneous melanomas over the last few decades.[2] Three most frequent primary skin cancers are basal cell carcinoma (BCC), squamous cell carcinoma (SCC) and malignant melanoma. Together SCC and BCC are referred to as nonmelanomatous skin cancers (NMSC). In India, skin cancers constitute about 1-2% of all diagnosed cancers. Basal cell carcinoma is the commonest form of skin cancer worldwide, but various studies from India have consistently reported SCC as the most prevalent skin malignancy.[3] Although complete data of incidence is not available, various cancer registries in India reported cumulative incidence of skin cancer varying from 0.5 to 2 per 100 000 population.[4] Although, the incidence of skin cancers in India is lower as compared to the Western world, because of a large population, absolute number of cases is estimated to be significant. In spite of being a surface malignancy and more amenable not only to early detection, but also to a potential cure, treatment outcome and follow-up data about survival is scarce from the Indian population. In this study, we present the disease profile and treatment outcome of patients treated at a tertiary care regional cancer centre who were with these three primary skin malignancies; namely SCC, BCC and melanoma. Various surgical procedures carried out and the importance of reconstruction using skin grafts, local and regional flaps wherever required following radical excision of primary skin cancer, without compromising the recommended surgical margins has been highlighted. Materials and methods The computerised database of Surgical Oncology Department at a Regional Cancer Centre was reviewed retrospectively. Patient records of a total of 77 patients with skin malignancies, out of a total of 3154 surgically treated patients in the Department for various malignancies between 1995 and 2002 were analysed. Patients were first evaluated in the out patient clinic by a team of Surgical and Radiation Oncologists and they underwent treatment according to the protocol decided by the same team. Apart from history and detailed clinical assessment, the pretreatment work up included a chest X-ray and routine blood examination. Imaging studies (CECT/MRI) were used only in locally advanced lesions to assess the extent of local infiltration. In patients with melanoma, ultrasound of the abdomen was used to evaluate any visceral or lymph nodal metastases. And in patients with enlarged regional lymph nodes, fine needle aspiration cytology (FNAC) was carried out to look for regional spread. Operative procedures and width of surgical margins varied according to the histology and extent of local infiltration by the tumour. For BCC, local excision was carried out with a minimum margin of 0.5 cm. For SCC, minimum three-dimensional margin taken was 1 cm. For malignant melanoma, minimum margin taken was 2 cm. Comprehensive regional lymph nodal dissection was performed if there was evidence of nodal involvement. Prophylactic lymph node dissection was not performed in any of the patients. For patients with skin cancers (SCC or Melanoma) of the extremities, where the disease had completely encased the neurovascular bundle or infiltrated bones, amputations were performed. In patients where excision was previously done elsewhere and if margin status was not clear, re-excision of the scar tissue and tumour bed was carried out. For large surgical defects not suitable for primary closure, reconstructions using split skin grafts, local (transposition/rotational advancement) or regional (fasciocutaneous/myocutaneous) flaps were performed. Adjuvant postoperative radiotherapy (50 Gy/25# over 5 weeks) was given in cases of SCC/BCC with positive tumour margins, with locally advanced growths and in patients with positive nodal disease. After completion of treatment, all the patients were followed up at three monthly intervals to look for relapse of disease. The collected database was analysed using SPSS-9 (SPSS Inc., Chicago, USA) statistical software. Disease free, survival analysis was performed using the Kaplan-Meier method. Results Patient profile Distribution of primary sites involved is shown in [Table - 1]. Forty-two percent of patients had locally advanced growths with involvement of deeper underlying structures such as subcutaneous tissue, muscle, bone and neurovascular bundle. Twenty-five patients had regional lymph nodal involvement. Fourteen out of 43 patients with SCC (32.5%) and 11 out of 20 (55%) patients with melanoma required regional lymph nodal dissection. Treatment details Morbidity and mortality Histopathology Follow up and survival Discussion Various reports from India show wide variations in the incidence and types of skin cancer from different parts of the country. Neve first reported ′Kangri′ cancer in the Kashmir region in 1900. Khanolkar and Suryabhai described a new type of skin cancer - ′Dhoti cancer′in 1945.[5] Very few literatures have been published from India in the recent period.[6] The reported incidence of skin cancers in India is less than 1% of all cancers.[7] In this study, common skin cancers constituted 2.4% of patients surgically treated at a referral regional cancer centre. Although there has been no significant increasing trend in the age-adjusted incidence of skin cancers in Indian patients, but in the Western countries, the incidence of skin cancers, especially of malignant melanoma has been rising for the past 40 years.[8],[9] In the Western countries, a vast majority of skin cancers are NMSC, mainly BCC.[10],[11] However similar to various earlier studies from India,[5],[12] the current study also shows that the most common histologic type of skin cancers is SCC (55.8%). The biologic behaviour of skin malignancies varies widely. Basal cell carcinoma rarely metastasizes and has an excellent prognosis and survival, whereas melanoma can be one of the most lethal malignancies with a high propensity for regional and systemic spread. Squamous cell carcinoma has 2-6% incidence of distant metastasis.[13] Approximately 3-10% of patients with melanoma present with metastatic disease in the absence of a clinically demonstrated primary lesion.[14] Basel cell carcinoma usually occurs on sun-exposed areas [Figure - 2] and SCC most commonly appears on sun-damaged skin. Squamous cell carcinoma can also arise in the precursor lesions such as actinic keratoses, Bowen′s disease, leukoplakia, or chronic scars.[15] Melanoma arises most commonly on the skin of the back in men and on the lower extremities in women in Western countries,[10] whereas sole of foot is the most common site for melanoma among Indian patients [Figure - 3].[8],[16] Sole of foot was involved in 60% of patients with melanoma in the current study. However, the commonest site of involvement for all the three skin cancers in the current study was scalp and facial skin (40.2%). The most important investigation in a case of suspected skin cancer is a proper excisional biopsy.[17]. Because these tumours involve superficial structures most of these patients undergo inadequate surgical excision at primary care canters owing to the lack of awareness and surgical expertise. Inadequate clinical information pertaining to the stage of the disease and type of resection (size, depth and status of margins) may create dilemma about the need for resurgery at a referral centres. In the current study, 32 (41.5%) patients had undergone some form of intervention elsewhere. Out of these, 24 patients had undergone resection of the primary lesion before coming to this centre. We have carried out re-excision of the scar tissue and tumour bed in these patients. In 20 out of these 24 (83.3%) patients, residual tumour was identified in the re-excision specimen. This suggests that optimal surgical margin was compromised during the initial surgery at primary care canters. The possible factors for inadequate resection could be - lack of awareness and temptation to achieve a primary closure of defect owing to the lack of reconstruction expertise. Treatment strategies differ for these three groups. Although, surgery is the mainstay of treatment for all the three common skin cancers, the extent of surgery, both local and regional varies. Adequate surgery is most important to prevent recurrence and long-term cure rates for patients with recurrent lesions are significantly lower than those for patients with primary lesions. Also, recurrent skin cancer is more likely to metastasize.[18] Adequate surgical margin is very important, particularly for melanoma, where margin depends upon the thickness (depth of infiltration) of cancer.[19] Although, various treatment options have been advocated for NMSC, no randomised, prospective study has compared treatment methods.[20] Simple surgical excision is effective for all types of BCCs. The cure rate approaches 99% when the histological margins are clear. Recommended margin is 5 mm; recurrence is more when the margin of resection is less than 4 mm.[15],[21] Moh′s micrographic surgery has been implied for recurrent lesions or those located in vital areas such as eyelid, digits, penis, nose, etc., but it requires a dedicated surgeon pathologist and onsite facility for pathology examination which is not present is most of the centres. For SCC, including locally advanced and recurrent tumours surgical excision is the mainstay of treatment.[15] At least a 1 cm margin beyond the apparent limit of the tumour is recommended. With the approach of taking proper recommended margins, we could achieve good local control for both BCC and SCC. In the current study, none of the patients with BCC developed local recurrence, whereas only one patient with SCC had local relapse. Regional lymph node dissection has no role in BCC, but in the presence of positive regional lymph nodes, therapeutic lymph node dissection is indicated for SCC.[7] We have carried out regional lymph node dissection in 14 patients with SCC. The mainstay of treatment for melanoma is surgical excision, with margins being determined by the depth of the tumour. Excision should include skin, subcutaneous tissue up to the muscle fascia.[22] Various trials have addressed the issue of margin.[11] The results of these studies suggest that a 1-cm radial margin is adequate for primaries with thickness up to 1 mm and 2 cm margin is adequate for primaries up to 4 mm thickness. None of these studies have shown that wider margins are necessary or related to improvement in survival. Although patients with primaries more than 4 mm thickness have a relatively high (approximately13%) risk of local recurrence, there are few data to support the use of margins wider than 2 cm.[22] In this study, margin of excision taken for melanoma was 2 cm because in most of these patients either the thickness of tumour was unknown (if excision biopsy was done elsewhere) or thickness was more than 1 mm. We could achieve good local control, with this strategy and only one out of 20 patients with melanoma developed local recurrence. In addition, control of regional spread is an important part of surgery for melanoma because it has a high propensity for early regional nodal spread.[19] In the current study, 11 out of 20 patients (55%) with melanoma underwent regional lymph nodal dissection and all had tumour detected in the nodal specimens. We could not perform sentinel node study routinely because most cases were either recurrent, previously inadequately treated or clinically node positive. Surgical margin and possibility of requirement of reconstruction are directly related to each other and there is always a critical trade off between them. Any compromise of the adequacy of surgical margin increases the chances of recurrence. A reconstructive procedure is always preferred to a potentially suboptimal surgical excision.[23] We had a liberal approach towards reconstruction of the surgical defects. We have carried out some form of reconstruction in 55.8% of the patients. The primary defects were closed using skin grafts in 34.88% (15/43) patients and loco regional flaps were used in 65.12% (28/43) patients. Only three patients out of 77 had positive tumour margins. Hence, we feel that reconstruction expertise is necessary for proper management of skin cancers, particularly for locally advanced growths. The role of adjuvant therapy is limited in skin cancers. Although radiotherapy can be used as primary mode of treatment for BCC and SCC located at certain sites such as the nose, lip, eyelid and canthus, where surgery is either technically difficult or likely to yield poor cosmesis. Radiotherapy has a very limited role in the management of melanoma.[7],[24] Postoperative radiotherapy is indicated in patients with advanced lesions, positive margins, lymph node metastasis, in-transit metastases in melanoma and for palliation.[25] In this study, adjuvant radiotherapy to local and/or regional sites was given in 27.2% patients for the indications mentioned earlier. Adjuvant chemotherapy and immunotherapy is generally used in advanced stage melanoma but results show only limited success.[9],[26] None of the patients in this study received chemotherapy or immunotherapy. In the current study, the rate of loco-regional disease relapse was 12.9% and 5-year median disease-free survival in the study population was 75%. These results suggest that it is possible to achieve reasonably good loco-regional control of disease with optimal surgery taking adequate margins and a reconstructive surgical procedure when needed. Conclusions Skin cancers constitute a small but significant proportion of patients with cancer. Unlike in the Western countries, SCC is the commonest histologic variety. Primary level inadequate intervention is very common. Good results can be obtained with radical surgery and optimal surgical margins along with a reconstructive procedure when needed.References
Copyright 2005 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn05025t3.jpg] [cn05025t2.jpg] [cn05025t1.jpg] [cn05025f2.jpg] [cn05025f3.jpg] [cn05025f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}