 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
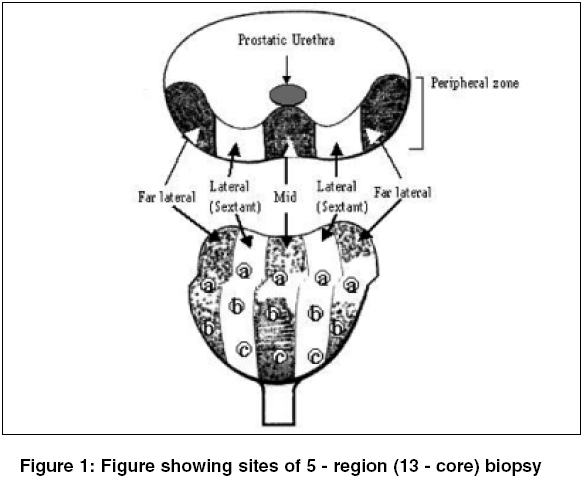
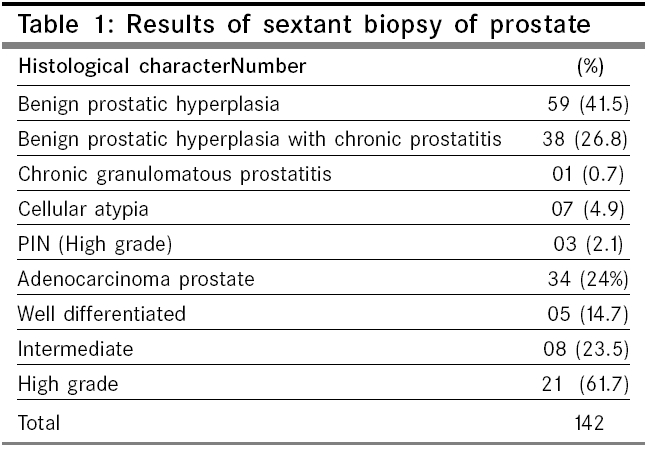
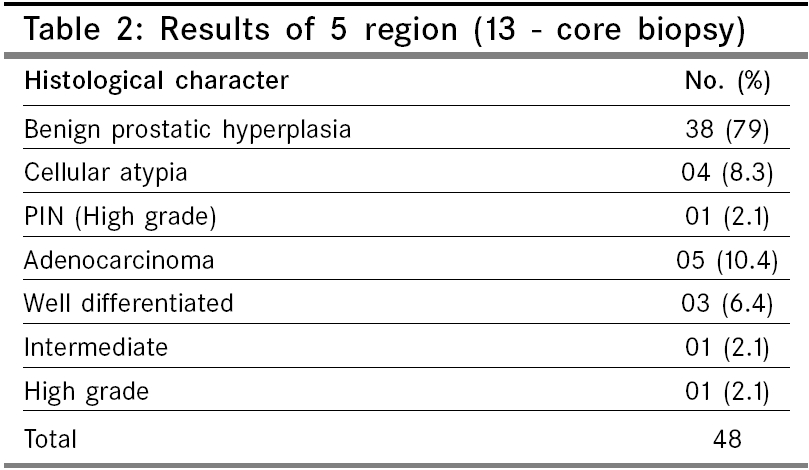
Indian Journal of Cancer, Vol. 42, No. 3, July-September, 2005, pp. 151-154 Original Article Transrectal ultrasound guided biopsy for detecting early prostate cancer: An Indian experience Gupta NP, Ansari MS, Dass SC Department of Urology, All India Institute Of Medical Sciences, New Delhi-110029 Code Number: cn05026 Abstract BACKGROUND: With the advent of prostate specific antigen the number of patients undergoing prostate biopsy has dramatically increased. The sextant biopsy technique has been conventionally used for the diagnosis of prostate cancer. Recently, concern has arisen that the original sextant method may not include an adequate sample of the prostate, hence it may result in high false negative rates. We conducted a prospective study to determine whether the 5-region prostate biopsy technique significantly increases the chance of prostate cancer detection as compared to the sextant biopsy technique.AIMS: To evaluate the efficacy of TRUS guided sextant and 5-region biopsy techniques in detecting carcinoma prostate in patients with PSA between 4 and 10 ng/ml and normal digital rectal examination. METHODS AND MATERIAL: Between December 2001 and August 2003 one forty-two men, aged 49-82 years, who presented with LUTS, normal digital rectal examination (DRE) and PSA between 4 and 10 ng/ml underwent TRUS guided sextant prostate biopsy. Serum PSA was reassessed after 3 months in patients whose biopsies were negative for cancer. If PSA was still raised, the patients underwent extensive 5-region biopsy. RESULTS: Mean patient age was 64 years and median PSA was 6.9 ng/ml. TRUS guided sextant biopsy revealed adenocarcinoma prostate in 34 men (24%). Median Gleason score was 7. Seven men (4.9%) had cellular atypia and 3(2.1%) had prostatic intraepithelial neoplasia (high grade). On repeat PSA estimation after 3 months, 48 patients showed stagnant or rising trend for which they underwent TRUS guided 13-core biopsy. Five (10.4%) patients were detected to have adenocarcinoma on repeat biopsy. Biopsy negative patients are on regular follow up with yearly PSA estimation. Complications included transient mild haematuria in14 patients (9.82%) and haematospermia in 4 (2.8%). Urinary retention developed in one patient and required an indwelling catheter for 4 days. CONCLUSION: Transrectal ultrasound guided sextant biopsy has shown a false negative rate of approximately 11%. A repeat 5- region (13-core) biopsy strategy can decrease the false negative rate of conventional sextant biopsy in patients with previously negative biopsies but persistently high PSA levels, high grade PIN or cellular atypia. Keywords: Prostate specific antigen, Prostate cancer, Prostate biopsy, Transrectal ultrasonography, Sextant biopsy Introduction With the increasing use of prostate specific antigen (PSA) estimation for diagnosing prostate cancer it has become necessary to have effective and sensitive methods of prostate biopsy 1-3. Since the introduction of sextant prostate biopsy by Hodge et al 1 in 1989, transrectal systematic sextant biopsies have been widely performed and up to 76% of American urologists use the sextant biopsy technique for detecting prostate cancer 2-5. Inspite of routine practice of transrectal ultrasound (TRUS) guided prostate biopsy in the west, similar data in Indian counterparts are sparse. We report our experience of TRUS guided sextant biopsy as well as extensive 5-region biopsy protocol in raised serum PSA and DRE (Digital rectal examination) negative patients.Materials And Methods From December 2001 to August 2003, all men older than 49 years who presented to our clinic with lower urinary tract symptoms (LUTS) underwent serum PSA measurement. Out of 212 patients, 142 had serum PSA between 4-10 ng/ml, which were included in the study and the remaining 70 patients had serum PSA >10 ng/ml. The inclusion criteria were serum PSA between 4-10 ng/ml, DRE negative, and negative digital guided random trucut biopsy. This was a prospective study and all the patients underwent TRUS guided sextant biopsy as an office procedure. The local ethical committee approved the study and informed consent was taken from all the patients. Before biopsy all patients had urine culture and anticoagulant therapy, if any, was stopped 7days before the procedure. Antibiotic prophylaxis of ciprofloxacin and tinidazole combination was started the same day and administered twice a day for 3days after biopsy. A cleansing enema was given the same morning. Visual analogue pain score (VAS) ranging from 0 to 10 was explained to each patient before starting the procedure 6,7. The patients were asked to grade the pain (0 to 10) at completion of the procedure. Based on these gradings the patients were subsequently divided in three groups; no pain (score 0-1), moderate pain (score 2-5) and severe pain (score 6-10). Twenty ml of 2% lidocaine jelly (Wockhardt Ltd., Bombay) was instilled per rectally 10 minutes before the start of the procedure. TRUS and sextant biopsy were performed in left lateral position by using 7.5 mega hertz monoplaner transrectal probe and HDI 5000 (Phillips medical system, USA) ultrasound machine. Spring driven biopty gun (Microvasive 18G/20cm) was used along with biopsy guide. Additional core biopsies were taken along with sextant if any hypoechoic areas were seen. All specimens were kept in individual bottles with 10% formalin and labeled separately. To unload the specimen biopty gun was directly fired in to specimen vial in order to save time. Patients whose sextant biopsy was negative underwent serum PSA estimation after 3 months and if still found high underwent 13-core extensive biopsy protocol. Criteria for 13-core biopsy protocol were biopsy negative patients with persistently high serum PSA, high grade PIN, cellular atypia. Biopsy negative patients were reviewed after 1 year. Procedure for 13-core biopsy was same as sextant biopsy except taking 2 cores from each anterior horn and 3 cores from mid line [Figure - 1]. Biopsy associated complications were recorded as insignificant or minor (pain during voiding, low grade fever, transient heamaturia or mild haematospermia) and significant or major (gross heamaturia, rectal bleed or bacteremia requiring admission)Results Mean patient age was 64 years (range 49-82). Median serum PSA was 6.9 ng/ml. After sextant biopsy adenocarcinoma prostate was detected in 34 of 142 men (24%), while 7 (4.9%) had cellular atypia and 3 (2.1%) had prostatic intraepithelial neoplasia (high grade). In 97 patients no cancer was diagnosed and biopsy was compatible with benign prostatic hyperplasia and/or prostatitis. One patient had granulomatous prostatitis [Table - 1]. Among the patients who had cancer the median Gleason score was 7. Well-differentiated adenocarcinoma (Gleason score-2 to 4), intermediate grade (Gleason score-5 to 6) and high grade (Gleason score-7 to 10) were identified in 5 (14%), 8 (24%) and 21 (62%) cases respectively. Pain visual analogue score was no pain (score, 0-1) in 12%, moderate pain (mean score-3, range 2-5) in 83% and severe pain (mean score-6, range 6-10) in 5% patients. One hundred seven patients who had negative biopsies underwent repeat serum PSA estimation after a course of antibiotics at 3 months. Fifty-nine patients (55%) showed a downward trend in serum PSA, hence repeat biopsy was not done. Forty-eight patients showed stagnant or rising serum PSA, for which they underwent 13-core biopsy. Five patients out of 48 (10.4%) were detected to have adenocarcinoma on repeat biopsy, which included one each from cellular atypia and high grade PIN group [Table - 2]. The false negative rate of sextant biopsy was 11%. Biopsy negative patients are on regular follow up and undergoing serum PSA estimation at one year and repeat biopsy after one to one and a half year. Complications included transient mild hematuria lasting for 1 to 4 days in 14 patients (9.82%) and haematospermia lasting up to 2 months in 4 (2.8%). Urinary retention developed in one patient requiring an indwelling catheter for 4 days. None of the patients had significant complication and required admission after the procedure. Discussion Diagnosis of prostate cancer requires obtaining cancerous tissue from the prostate gland with biopsy. The advent of transrectal ultrasound has revolutionized prostate biopsy techniques, which has greatly increased the diagnostic accuracy of biopsy. With more than 175,000 new cases of prostate diagnosed each year, and with many more patients biopsied to rule out carcinoma, transrectal ultrasound with prostate biopsy has become a commonly performed urological procedure in USA. Introduced by Hodge et al in 1989 the sextant prostate biopsy has been the gold standard for diagnosing prostate cancer 1. Absolute indications for prostate biopsy include (i) Serum PSA greater than 4 ng/ml 2 (ii) Abnormal digital rectal examination 3 and (iii) Presence of high grade PIN or cellular atypia on prostate biopsy 4. The addition of prostate specific antigen (PSA) as a screening tool for prostate cancer has increased the application of transrectal ultrasound and prostate biopsy. Different methods have been proposed to increase the specificity of PSA when it is between 4-10 ng/ml including age specific PSA, PSA density (PSAD) and percent free PSA (% fPSA) 8,9. Percentage free PSA and PSAD both provide comparable results, which are better than age specific PSA 9,10. It has been suggested that % fPSA may be used instead of PSAD to decide a repeat biopsy as former does not require ultrasonography 8. As originally described in the sextant method 6 biopsies of prostate are taken, with specimens obtained from the base, middle and apex of the prostate in the mid lobar parasagittal planes bilaterally 1. Although the sextant method was the first described systematic method of prostate biopsy, other methods have demonstrated that the sextant technique as originally described has a false negative rate up to 30 % 11 (11% in the present study). This false negative rate is understandable as this method not only involves taking fewer cores, but also samples a smaller percentage of the peripheral zone of prostate where only 80 % of prostatic adenocarcinoma is found. More recently the sextant method has been modified to include more laterally directed biopsies 12. These biopsies, which have been described as "lateral biopsies" in several studies, include areas of prostate that have been referred to as the "far lateral region" and "anterior horn". Multiple in-vivo studies have revealed that increasing the number of prostate biopsies enhances prostate cancer detection 13-17. Because the cross sectional anatomy of the prostate demonstrates an almost 3 fold increase in the peripheral zone of the lateral prostate compared with other areas of the gland, a more extensive method of biopsy was developed to sample the lateral areas more thoroughly. The 5-region method involves obtaining cores from the traditional sextant regions (6 cores) as well as 4 cores (2 from each side) from the far lateral regions "anterior horn" and 3 mid line biopsies [Figure - 1]. By increasing the number of peripheral zone biopsies, the 5-region technique decreases the false negative rate by 35% 14. Eighty-eight percent of the additionally detected cancers are found in the far lateral areas of prostate gland, which are composed entirely of peripheral zone tissue 18. Norberg et al (1997) in a prospective study of 512 patients observed that eight-core biopsy i.e. sextant biopsy with two additional lateral biopsies detected more cancer than the conventional sextant biopsy 18. Brossner et al (2000) in a retrospective study reported an additional 29% cancer detection with 12-core biopsy in comparision to traditional sextant biopsy 19. Similarly Presti et al (2000) reported higher cancer detection rates of 9% and 14% with 8- core and 14-core biopsy 16 . More recently Eskicorapci et al (2004) showed that additional four biopsies from the lateral peripheral zone along with sextant technique increases the cancer detection rate by approximately 10% 20. In an interesting study from Asian subcontinent which is considered to have a low prevalence of prostate cancer has shown an almost twice cancer detection rate with the increase in numbers of biopsies i.e. 8-14 cores 15. In our study the sextant biopsy picked up initially 24% cancer and on subsequent follow up 13-core biopsy detected another 10.4% of cancer. Lastly, the morbidity associated with taking more biopsy cores does not increase significantly 15, 21. In the present study most of the complications were self-limiting as none of the patient had significant complications like gross haematuria, rectal bleed or bacteremia warranting hospitalization. Conclusion Transrectal ultrasound guided sextant biopsy once the gold standard method of prostate biopsy, has shown a false negative rate of approximately 11%. A repeat 5- region (13-core) biopsy strategy can decrease the false negative rate of conventional sextant biopsy in patients with previously negative biopsies but persistently high PSA levels, high grade PIN or cellular atypia.[21]References
Copyright 2005 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn05026f1.jpg] [cn05026t1.jpg] [cn05026t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}