 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
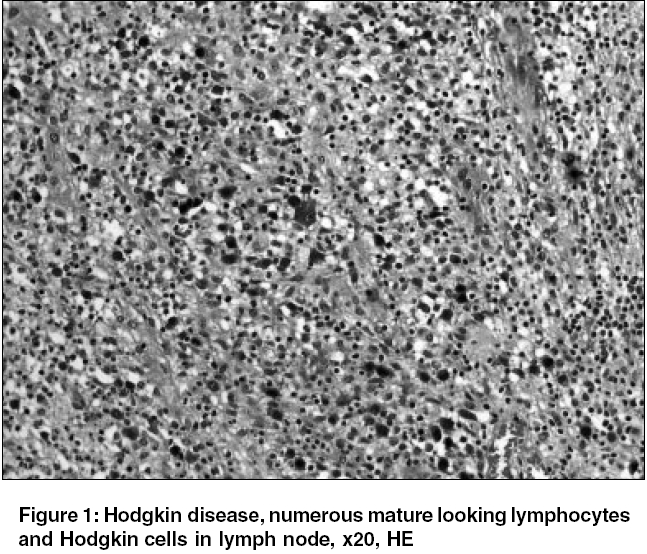
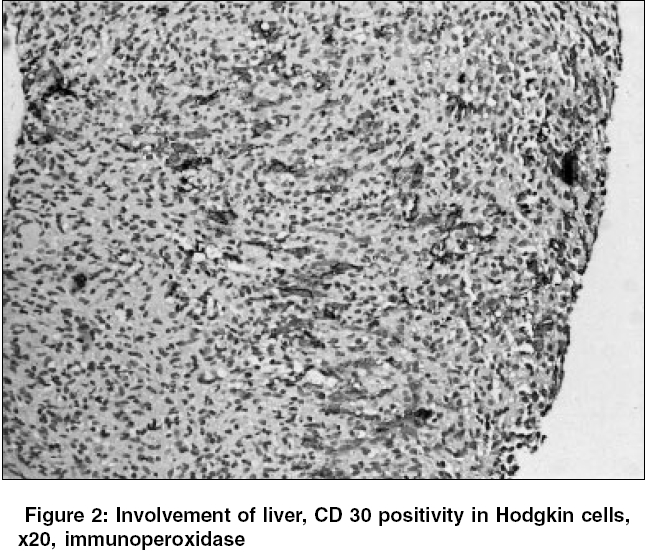
Indian Journal of Cancer, Vol. 42, No. 3, July-September, 2005, pp. 158-160 Case Reports Hodgkin's disease in an elderly patient with B-Cell chronic lymphocytic leukemia Colak Dilsen, Ozyilkan Ozgur, Akcali Zafer, Bilezikci Banu Baskent University Faculty of Medicine Department of Medical Oncology and *Pathology, Ankara Code Number: cn05028 Abstract Chronic lymphocytic leukemia (CLL) is the most common type of leukemia worldwide. It is an indolent disease, almost exclusively of B-cell origin. Some CLLs evolve into a more aggressive lymphoid malignancy. The most common of these is Richter's syndrome. Transformation to acute lymphoblastic leukemia, plasma cell leukemia, multiple myeloma, or Hodgkin's disease (HD) may also occur. CLL patients are also at a significantly increased risk of developing a second malignant neoplasm later in life. One of the most common of these is HD. Herein, we report a case of HD in an elderly man with a history of B-cell CLL.Keywords: Chronic lymphocytic leukemia, Hodgkin disease, Secondary neoplasm, Richter′s syndrome Introduction Chronic lymphocytic leukemia (CLL) is a clonal lymphoproliferative disorder characterized by an increased number of morphologically mature appearing but immunologically incompetent lymphocytes in the peripheral blood, bone marrow, spleen, and lymph nodes. It is an indolent disease, almost exclusively of B-cell origin, occurring in middle to late adulthood.[1] Approximately 3% to 15% of CLLs evolve into a more aggressive lymphoid malignancy. The most common of these is Richter′s syndrome. Anecdotal reports have been published of a transformation to acute lymphoblastic leukemia, plasma cell leukemia, multiple myeloma, or Hodgkin′s disease (HD).[2] CLL patients are also at a significantly increased risk of developing a second malignant neoplasm. A significant number of cases have been reported for cancers of the lung, brain, and eye, as well as malignant melanoma and HD. In patients with B-cell CLL, there is an approximately 8-fold increased risk of HD, with HD representing one of the most frequent secondary neoplasms.[3] In our case, HD occurred when the CLL was in remission. There were only a few reported cases in this group, and our case represents 1 of the very rare associations of HD with CLL.[4] Case History In December 1994, a 58-year-old man was admitted to the hospital because of a palpable mass in his left upper quadrant. On physical examination, the liver was palpable 4 cm below the right costal margin and the spleen was palpable 16 cm below the left costal margin. The patient was anemic (hemoglobin level, 8.9 g/L), with a platelet count of 134,000/L, a leukocyte count of 21.8 x 109sub/L, and an absolute lymphocytosis (90%). Evaluation of a peripheral blood smear and bone marrow biopsy confirmed the diagnosis of B-cell CLL. Clinical Rai stage was III. Single-agent chemotherapy with chlorambucil (10 mg/day) was initiated. No satisfactory clinical response was observed, and leucopenia developed. In February 1995, radiotherapy to the splenic area was applied, and a combination protocol of cyclophosphamide, vincristine, and prednisone (CVP) was started. At the end of the sixth cycle of CVP, a complete response was obtained. The patient was off therapy and asymptomatic until September 2001, when he came to the hospital with a rapidly growing left inguinal lymphadenopathy. Excisional biopsy of the inguinal lymph node showed Hodgkin′s/Reed-Sternberg cells with classical morphologic features. He was diagnosed and staged as mixed-cellularity Hodgkin′s disease, stage IA. He was treated with a combination protocol of adriamycin, bleomycin, vinblastine, and dacarbazine (ABVD) for 3 cycles, and then regional inguinal radiotherapy was applied. The disease progressed however. The lymph nodes in inguinal region increased in number and size. Abdominal CT scan showed multiple hypodense masses in the liver, suggesting metastases. Pathological examination of Tru-cut biopsy specimens of the mass in the liver revealed Hodgkin′s lymphoma infiltration. Immunohistochemical studies demonstrated that the Reed-Steinberg cells expressed CD15 and CD30, but did not express CD3 or CD20. A COPP regimen (cyclophosphamide, vincristine, procarbazine, prednisone) was planned, but the patient died at home before treatment could be started. Discussion Occurrence of HD in CLL, although rare, is considered one of the most common secondary neoplasms in patients with a previous history of B-cell CLL. It is unclear whether these two diseases are related one to another. HD in CLL may be due to a clonal transformation from CLL or it may occur as a de novo secondary neoplasm. The occurrence rate of HD in CLL patients has been reported to be around 0.5%.[3] In these cases, major points of interest are the clonal relationship between CLL and H/RS cells, clinical implication of this diagnoses, prognosis, and treatment.[5] The prognosis and treatment of HD in CLL patients are still not clear. The prognosis and treatment may be different in cases of "CLL with Hodgkin′s transformation" and de novo HD. This is not clear in the literature. It has been suggested that HD transformation in CLL patients is probably characterized more by poor response to therapy and short survival. [6],[7] However, there have been studies suggesting good prognoses also.[8],[9],[10] Adiga and colleagues analyzed data from 88 cases with an initial diagnosis of B cell-CLL followed by subsequent development of HD and found that prognosis was poorer in patients with continued active CLL when compared with those whose CLL was in remission at the time of HD occurrence. In our case, HD occurred when the CLL was in remission. There were only 5 reported cases in this group, and our case represents 1 of the very rare associations of HD with CLL.[4] There is no consensus about the most effective chemotherapy regimen for CLL transformation to HD. MOPP, ABVD, and BCVPP with or without RT are the frequently used chemotherapy regimens. In our case, we first chose the ABVD regimen, but no response was observed. Then we planned to institute the COPP regimen, but the patient died before the treatment could be started. Because the reported cases are relatively small in number, the data are far from conclusive, and the prognosis and treatment of HD in CLL remain to be established. References
Copyright 2005 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn05028f2.jpg] [cn05028f1.jpg] |
| |||||||||

{kind=link}
{kind=link}