 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 42, No. 4, October-December, 2005, pp. 178-184 Original Article Quality of life of head and neck cancer patient: Validation of the European organization for research and treatment of cancer QLQ-C30 and European organization for research and treatment of cancer QLQ-H&N35 in Indian patients Chaukar DA, Das AK, Deshpande MS, Pai PS, Pathak KA, Chaturvedi P, Kakade AC, Hawaldar RW, DCruz AK TATA Memorial Hospital, Parel, Mumbai, India Code Number: cn05032 Abstract Aims: To present the first cross-culture validation of the European
organization for research and treatment of cancer (EORTC) quality of
life questionnaires, the EORTC-QLQ-C30, and the QLQ-H&N35 in India.
Settings and Design: These questionnaires were translated into two vernacular languages and pilot test was done on 15 patients. Two hundred head and neck cancer patients completed the QLQ-C30 and the QLQ-H&N35
at two time points during their treatment. Psychometric evaluation of the structure,
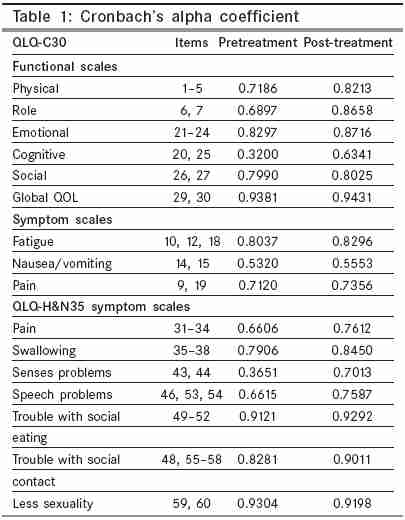
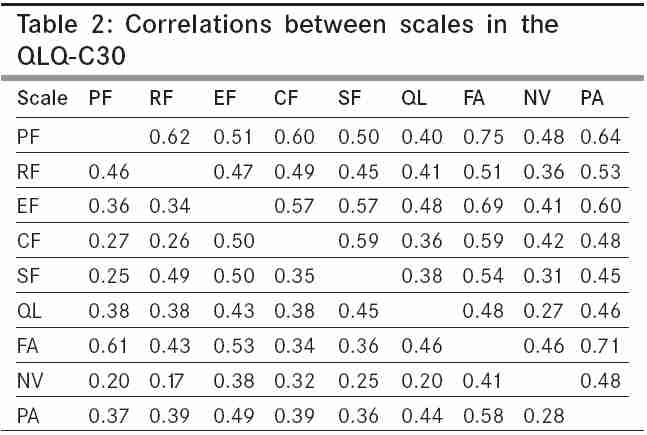
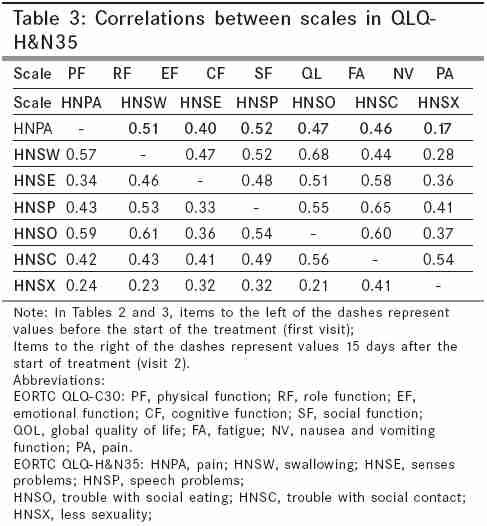
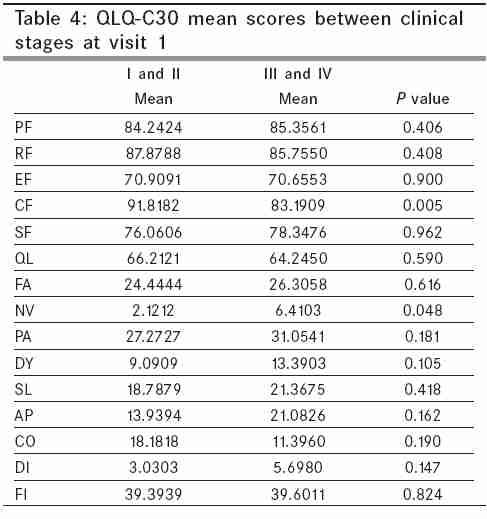
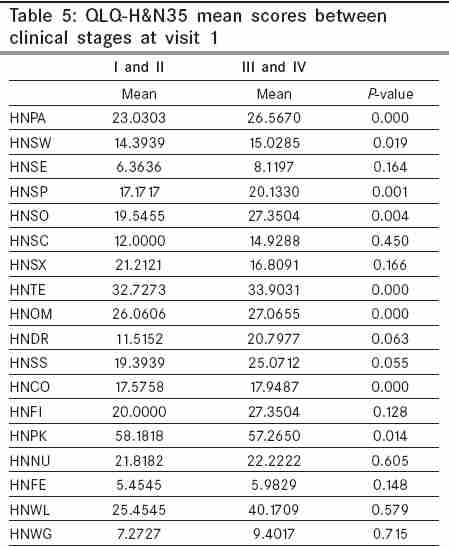
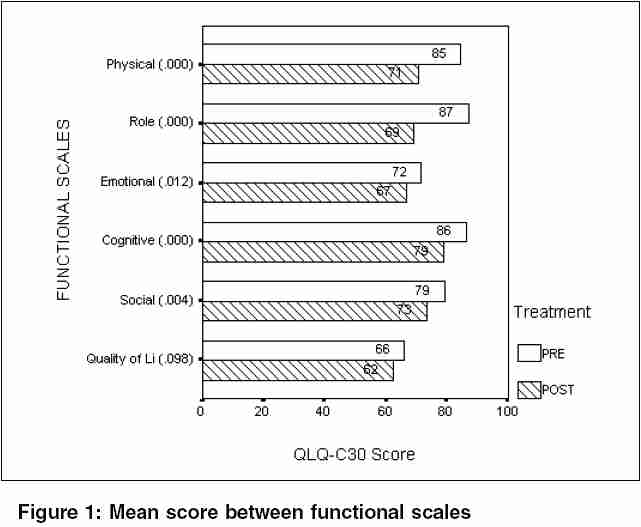
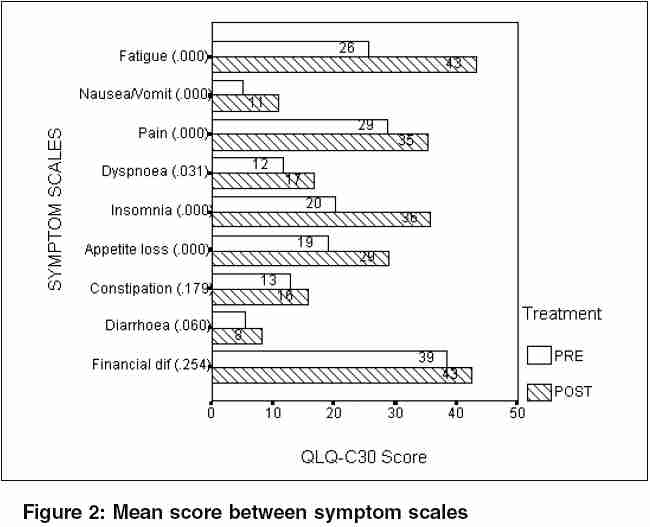
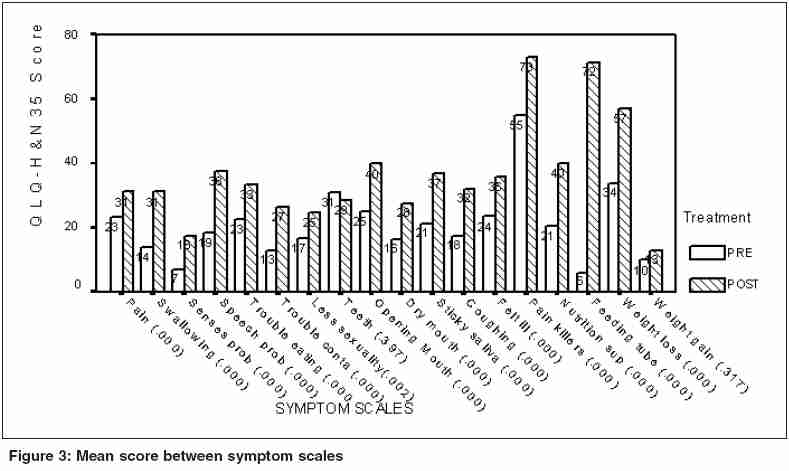
reliability, and validity of the questionnaire was undertaken. Keywords: Head and neck cancer; quality of life; validation. Cancer outcomes are traditionally measured in terms of overall survival, disease free survival, time to disease progression, and other disease variables. Although these outcomes remain essential, there is general recognition of the need to assess the impact of cancer, and its treatment on patient′s health-related quality of life (HRQOL). [1],[2],[3] The field of HRQOL has burgeoned in the past two decades. Inclusion of HRQOL measure in medical research is common in the West,[4] but there are few studies from developing countries. The questionnaires measuring QOL have been developed in the western countries, which are culturally different from India. Head and neck cancer is a major health problem in India as opposed to the West, where it accounts for only 5% of all cancers. Also, head and neck cancers are mainly seen in the low socio economic strata, making it difficult to apply the same quality of life parameters measured in the developed countries with better standards of living. So far, there are no longitudinal studies on QOL reported from India. Although illiteracy and poverty are the often-cited reasons for our neglect toward measurement of QOL, it is actually the lack of physician awareness, and the nonavailability of valid tools that are responsible for the paucity of QOL studies in India. Moreover, India is a country of 27 official languages, making the translation procedure difficult. Hindi is the national language and is spoken by a large number of patients. Hence, it was advisable to translate the questionnaire into Hindi and Marathi (the local language of the state of Maharashtra). India is a developing country with a literacy rate of only 57%.[5] Most of our patients are socio-economically backward and would accept the treatment decided by the physician. Needless to say that the various treatment options and alternatives are seldom discussed. Most of them are too scared to report emotional, mental, and physical problems. In such a scenario, the onus lies on the physician to study treatment effects and try, and improve patients QOL. A modular approach is necessary to assess the multidimensional aspects of QOL. A general module, which assesses symptoms commonly experienced by cancer patients, is supplemented by a site or treatment-specific module, which assesses difficulties unique to that particular type of cancer. Such an approach is embedded in the questionnaire developed by the European Organization for Research and Treatment of Cancer (EORTC), which is the most widely used questionnaire. The present study was undertaken to use and validate the EORTC QLQ-C30 (core questionnaire) and the QLQ-HN35 (head and neck-specific questionnaire) into two vernacular languages (Hindi and Marathi), and we present the first validation of these questionnaires in head and neck cancer patient population in a tertiary cancer center in India. Patients and methods Patients Instrument The questionnaire was served twice. Once preoperatively and again at the 15th postoperative day, giving a total of 400 filled questionnaires. A study co-ordinator, not concerned with patient care, served the questionnaires and the patients were asked to fill and return the questionnaire within 48 hours. The questionnaires were checked and corrected for missing values in the patients, presence. The relevant clinical details including age, gender, level of education, site, and stage of the tumor, and the surgical details were recorded from the hospital case files. Assessment of validity Reliability Construct validity Within scale correlation Between scale correlation Criterion validity Responsiveness Statistical analysis Results Before commencing the study the translated questionnaire was pilot-tested on 15 patients. The average time to fill the QLQ-C30 was 8 minutes and for QLQ-H and N35 it was 7 min. The patients found it easy to fill and no major changes were necessary. Two hundred patients completed the questionnaire pre- and postoperatively, giving a total of 400 completed questionnaires. Thirty-three patients filled the English version whereas 167 (83.5%) patients filled the translated vernacular version (104 Hindi, i.e., 52%; 63% Marathi, i.e., 31.5%). Except for a brief explanation of the purpose, content, and layout of the questionnaire, most patients were able to complete the questionnaire without assistance. There were 148 (74%) males and 52 (26%) females. One hundred and thirty two patients (66%) had completed their education at least till matriculation. The site of primary tumor was the buccal mucosa and the gingivo buccal sulcus (52%), tongue and floor of mouth (16%), larynx and hypopharynx (12.5%), thyroid (12.5%), and maxilla (3%). Miscellaneous tumors including tumors of the salivary gland and neck nodes metastasis of unknown origin (MUO) were grouped together (4%). Fifty-five patients (27.5%) had early-stage tumor (I and II), whereas 117 (58.5%) patients presented in an advanced stages (III and IV). Twenty-eight patients (14%) (thyroid, salivary glands, MUO) could not be staged as per the TNM classification. Reliability Cognitive functioning and the nausea vomiting scale (QLQ-C30) demonstrated a low alpha coefficient at both visits whereas head and neck senses scale (H& N35) demonstrated a low value at the first visit. Construct validity Clinical validity-known-group comparisons Patients with oral cancer reported higher problems with the teeth, mouth opening, pain, and social contact as compared with patients with laryngeal and hypo-pharyngeal cancers who reported higher problems with speech and cough. Responsiveness In the QLQ-H&N35 there was a statistically significant deterioration in the post-treatment scores as compared with the pretreatment scores for all the scales, except for problems with teeth and weight gain [Figure - 3]. Discussion Head and neck cancer is a major health problem worldwide. It is a bigger problem in developing countries like India, where it accounts for 30% of all cancer in males, and 13% of cancer in females.[7] At the Tata Memorial Hospital, which is a tertiary cancer center, it accounts for approx 25%[8] of the patient load. The head and neck region includes numerous delicate, intricately organized structures essential for basic physiological functions, and critical for appearance, expression, and social interaction. Depending on the site, size, and patterns of spread, head and neck tumors can cause varying degrees of structural deformations, and functional handicaps compromising well-being, self-esteem, and social integration. In addition, treatment of head and neck tumors can induce additional mutilation, thereby worsening the quality of life. Hence, QOL is an important end-point in evaluating treatment results of head and neck cancers. In planning a study that proposes a standardized evaluation of the impact on QOL of a treatment, two options are available. The first involves designing an instrument ex novo . However, this is not an easy solution, because a new instrument can be used in a clinical study only after a validation procedure, which may take four to six years.[9] The second option requires us to translate one of the existing and validated instruments, the majority of which are in English. This study is the first to translate and validate the EORTC-QLQ-C30 and the QLQ-H&N35 modules for use in the Indian population with head and neck cancer. The advantage of translating a validated tool into a local language instead of developing a new one is primarily the amount of time that is needed to establish the reliability for the translated tool. The present study was performed to test the applicability of a western questionnaire in a different cultural background like ours and also to validate the translated version. Once the questionnaire is validated, it can be used for multicentric studies across the nation. We are presenting the results of a validation study of the EORTC-QLQ-C30 and the QLQ-H & N35 questionnaire in Indian patients with head and neck cancer. The translations were performed according to the guidelines laid down by the EORTC. Because of familiarity with English language in our country, we did not encounter much difficulty in the translation procedure and we could frame the sentences with the same meaning as the original version. In most instances the translated versions were a mirror image of the original version. The translated versions were pilot- tested on 15 patients. This is an essential step in cross-culture validation as it gauges the acceptability of the questionnaire. The original and the translated versions were tested for psychometric properties. Both the scales demonstrated acceptable reliability. The internal consistency coefficients of all scales of the EORTC-QLQ-H&N35 were satisfactory (>0.70). In the QLQ-C-30, the cognitive function and the nausea and vomiting scale had a low alpha coefficient at the first visit, which improved at the second visit. Similar findings have been reported on other studies.[10],[11] The cognitive function scale has also shown limitations in the first assessment of the EORTC validation study (α = 0.56)[12] The low internal consistency coefficient in cognitive function, nausea, and vomiting might have resulted from the diversity of the patient conditions. In both the questionnaires, the items correlated with their respective scales and did not show a high correlation with any other scale. The small-to-moderate correlation between scales from the QLQ-C30 and the QLQ-H&N35 indicate that the two modules tap relatively different dimensions of QOL, as intended. Within the core questionnaire (QLQ-C30) the physical functioning and the pain scale correlated with the fatigue scale at the second visit. This can be explained by the fact that clinically the items measuring these scales are linked and correlate with each other. The tests for validity based on comparisons between patient subgroups known to differ in clinical status yielded generally consistent results. The QLQ-C30 was less successful in discriminating between patients with different stages of disease. The H&N35 was more sensitive in detecting the difference in symptoms for early- vs advanced-stage disease. An essential property of QOL instrument intended for use in clinical trials is that it should be responsive to changes in patients′ health status over time. In the current study, statistically significant changes in functional and symptom levels were observed in the expected direction. Postoperative patients had a significantly worse score in most of the scales as compared wirh preoperative patients. We conclude that the EORTC-QLQ-C30 and the QLQ-H&N35 have satisfactory psychometric properties when applied to a sample of Indian population with head and neck cancer. The translated versions have satisfactory levels of reliability and validity. The instrument can now be used for multicentric studies and can also be used in prospective clinical trials. References
Copyright 2005 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn05032t1.jpg] [cn05032f2.jpg] [cn05032t4.jpg] [cn05032t2.jpg] [cn05032t5.jpg] [cn05032f1.jpg] [cn05032f3.jpg] [cn05032t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}