 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
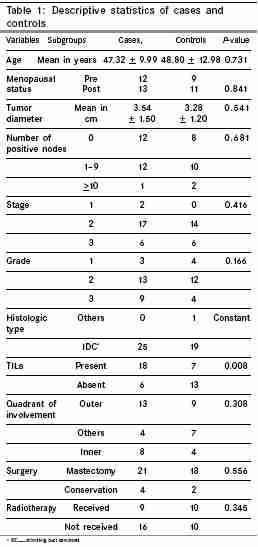
Indian Journal of Cancer, Vol. 42, No. 4, October-December, 2005, pp. 185-190 Original Article Effect of preoperative short-course famotidine on TILs and survival in breast cancer Parshad R, Hazrah P, Kumar S, 1Datta Gupta S., 2Ray R, 2Bal S Department of Surgery, All India Institute of Medical Sciences, New Delhi, India, 1Department of Surgery, Raja Muthiah Medial College and Hospital, Annamali University, Chidambaram, India, 2Department of Pathology, All India Institute of Medical Sciences, New Dehli, India Code Number: cn05033 Abstract Background: Histamine receptor antagonists have been shown to induce tumor-infiltrating lymphocytes (TILs) in colonic cancers and improve survival. The role of histamine receptor anatagonists in breast cancer is unclarified.Aim: To evaluate the role of histamine receptor antagonists in inducing (TILs) in breast cancer. Method: Forty-five patients with operable breast cancers (25 cases who received preoperative famotidine and 20 controls) were studied for the effect of famotidine in inducing TILs and survival in breast cancer. Results: Significant TILs were seen in 75% (18/24) of cases as opposed to 35% (7/20) controls. In logistic regression analysis the only variable found to be predictive of TILs was famotidine, odds ratio 7.324 (1.693-31.686) P = 0.008. In Cox's regression presence of TILs was favorably associated with improved disease free survival at a median follow up of 35.56 months. The hazard ratio for disease relapse was 3.327 (1.174-9.426) P = 0.024 in TIL negative as compared to TIL positive patients. Famotidine use alone was not significant in the original model, however, on incorporation of quadrant of involvement in addition to other established prognostic factors in the above multivariate model, it assumed borderline significance with a hazard ratio for disease free survival 3.404 (1.005-11.531, P = 0.049). Conclusions: Preoperative short course famotidine induces TILs in breast cancer. Patients with TILs demonstrable in tumor specimens had an improved disease free survival. Famotidine may improve disease free survival in breast cancer and these findings need validation in larger population subsets. Keywords: breast cancer; famotidine; survival; tumor infiltrating lymphocytes H2- receptor antagonists are being investigated for their possible immuno-modulatory role in malignancies, the concept having emanated after the phenomenal correlation, in which the coincidental use of H2- receptor antagonist to alleviate gastrointestinal symptoms led to regression of metastatic lesions in advanced malignancy.[1],[2] The postulated mechanisms by which histamine exerts its immunosuppressive effects have been various; most of these have been related to pathways modifying the response of tumor-infiltrating lymphocytes (TILs)[3],[4] and are mediated by H2 receptors, and therefore have been suggested to be reversible with H2-receptor antagonists. [3],[4],[5] Although the prognostic role of TILs is as yet not uniformly established, observations suggest that TILs may influence survival in cancers. [6],[7],[8] The beneficial effects of the H2-receptor antagonist cimetidine in inducing TILs and conferring a survival advantage have been largely confined to the realms of colonic cancers; [9],[10],[11] nevertheless, isolated reports of such an effect having been observed in other solid tumors also exist.[12] Other H2-receptor antagonists that have also been studied in this regard are ranitidine and famotidine. [13],[14],[15] Tsunodu et al . in 1991 have reported augmentation of cytotoxic activity of lymphocytes by famotidine in cancer patients in doses equivalent to antacid doses.[15] A recent study also demonstrates increased lymphocyte infiltration in colorectal cancers with the use of famotidine.[16] In a previous study conducted at our institution, Parshad et al .[17] had observed that famotidine, a H2-receptor antagonist, was effective in inducing TILs in breast cancer. The present study substantiates the above results in a larger population and evaluates the effect of famotidine and TILs on the course of disease in breast cancer patients. Materials and methods In the period from May 1998 to June 2002, 50 patients with nonmetastatic breast cancer who consented for the study had been randomized into two groups, viz. cases and controls, to study the effect of famotidine on TILs. Our analysis is confined to the findings in a subset of 45 of the above 50 patients, 25 cases (those who received preoperative famotidine), and 20 controls (those who did not receive the drug and refrained from the use of any such drug in the perioperative period). Patients who were excluded from the analysis (5/50) were as follows: Patients lost to follow-up early in the study ( n = 1), patients with second cancers ( n = 1) who also were detected to have mucinous adenocarcinoma of the gall bladder, and those who received neo-adjuvant chemotherapy ( n = 3). Interventions Two consultant pathologists who were blinded to case and control groups independently assessed the operated specimens for the following.
Antibodies used for immunohistochemistry For B cells-(CD 20), monoclonal antihuman CD 20 cy-clone L 26 directed against antigen L 26, Dakopatts (Dakocytomation, Denmark), A/S in 1: 50 dilution. All patients received post operative adjuvant systemic therapy (4 patients received hormone therapy only, 7 chemotherapy only, and 34 patients received both hormone and chemotherapy). Radiotherapy was administered whenever indicated. Patients were evaluated in the follow-up clinic with clinical examinations, X-ray chest, and serum alkaline phosphatase every 3 months for the first 3 years, every 6 months after 3 years till completion of 5 years, and yearly thereafter. In addition, patients were also advised a yearly routine mammogram and investigated with other imaging modalities whenever there was suspicion of disease relapse. The median follow-up of the study group is 35.56 months and the mean is 40.5 ± 18.6. A computerized grouped database was constructed using established prognostic factors and statistical analysis was done using the SPSS program. The equality of distributions of parameters between the groups was analyzed using nonparametric tests, viz., Wilcoxon rank sum and χ2 tests. A multivariate model was constructed and incorporated data on: age, menopausal status, pathological size of the tumor, number of lymph nodes involved, pathological stage according to AJCC fifth classifications, grade of the tumor, histologic type, type of surgery, i.e., conservative vs mastectomy, whether the patients received adjuvant radiotherapy, and one of the two exclusive criteria, i.e., whether the patient received famotidine or whether the specimen demonstrated TILs. All patients received adjuvant systemic therapy, which has therefore not been considered in the model. Age and tumor size were included as a continuous variable and others as categorical variables. Binary logistic regression analysis was done with all the above parameters other than the treatment variables of the multivariate model (i.e., extent of surgery and radiotherapy) to determine factors predictive of TILs. Survival analysis was done using Cox′s regression using stepwise selection with all parameters included in the above multivariate model. Both disease-free and overall survival were calculated from the date of surgery and the event in consideration was either local disease recurrence or distant relapse in the former and death owing to disease progression in the latter. There were no external sponsors or conflicts of interest attributable to any part of the study. The cost of the immunohistochemistry required for estimation of TILs and their typing was availed as a part of the institute grant. Results [Table - 1] shows the descriptive statistics of the patients in the two groups. Of the 45 patients included for the analysis, the estimation of TILs could not be done in one, as the sample was autolyzed. The above patient had received preoperative famotidine and has been therefore included in the survival analysis of the famotidine subgroup. No adverse effects were noted in any of the patients. The two groups were comparable regarding presenting parameters and histopathological tumor characteristics other than TILs. TILs were observed in a greater percentage of cases-the difference being significant. In logistic regression analysis, the only variable found to be significant in prediction of TILs was famotidine (odds ratio of 7.324 (1.693-31.686), P = 0.008). TILs, when present, did not vary in the location, i.e., periphery (stromal) or center (in intratumoral areas), among cases and controls. Famotidine use was predictive of both intratumoral [β= 10.605 (1.945-57.823), P = 0.006] and stromal [β = 5.600(1.484-21.127), P = 0.011] TILs in regression analysis. Age, menopausal status, tumor size, nodal status, histopathology, grade, and quadrant did not have any significant influence on TILs. Typing of the TILs could be done in 36 patients (19 cases and 17 controls). Among patients with significant infiltrations, in 18/19 cases the predominant type was T-lymphocytes. On the other hand, in patients with insignificant infiltrations, i.e., 14/17, the predominant infiltrate was also of the T-cell type. The mean percent of T- and B-lymphocytes was 81.842% and 18.158% in patients with significant infiltration, the difference being significant ( P =0.001). The predominant type in all patients except one was infiltrating duct carcinoma (IDC). One patient in the control group had invasive lobular carcinoma. In patients with IDC, some areas of cribriform type were seen in five cases, of colloid type in one, and lobular type in an other. There were no medullary carcinomas. No patient had DCIS alone. However, DCIS was present along with invasive ductal carcinoma in two cases and four controls. Five patients in cases (20%) had died owing to disease relapse whereas three were alive with recurrence (12%) and seventeen were disease-free (68%) at the time of the analysis. On the other hand, in the control group six patients (30%) had died owing to disease relapse, whereas three were alive with recurrence (15%) and eleven were disease-free (55%). In multivariate analysis using Cox′s regression, presence of TILs was favorably associated with improved disease-free survival. The hazard ratio for disease relapse was 3.327 (1.174-9.426); P = 0.024 in TIL-negative as compared with TIL-positive patients. Famotidine use alone was not significant in the original model; however, on incorporation of quadrant of involvement in the above multivariate model it assumed borderline significance with a hazard ratio of 3.404 (1.005-11.531, P = 0.049) for disease free survival in patients who did not receive famotidine as compared with those who received the drug. The hazard ratio for disease relapse in TIL-negative as compared with TIL-positive patients on inclusion of quadrant of involvement was 4.686 (1.375-15.976), P = 0.014. Comparison in univariate analysis (Kaplan-Meier curves) with consideration given for tumor location, separately for each quadrant, demonstrated that famotidine receivers had a significantly better survival than those who did not receive famotidine in patients with tumors in the outer quadrants The mean survival for the famotidine group was 60.35 + 5.59 months, whereas that in nonfamotidine group was 28.48 + 6.34; P = 0.0122, the difference being significant in log rank test. Other factors, i.e., the location of TILs stromal vs intratumoral or famotidine-TIL interaction strata did not emerge as significant. Discussion There are various reports demonstrating the beneficial effects of lymphocytic infiltration in human solid tumors. Variants of gastric carcinoma exhibiting lymphoid infiltration have a better prognosis.[18] Malignant melanoma heavily infiltrated with lymphocytes have been reported to undergo spontaneous regression.[19] Also, it is well known that medullary carcinoma of the breast which usually has demonstrable tumor-infiltrating lymphocytes has a favorable prognosis, although this histologic variant has other inherent characteristics, which by themselves would qualify it to be an aggressive tumor-like high grade and mitotic counts.[20] The cytotoxicity of TILs is reported to be mediated by two pathways: Perforin-induced membrane lysis, Fas-induced DNA fragmentation and apoptosis.[21],[22] Interleukin-2 has been a potent method of stimulation of activation and proliferation of TILs.[23] Enhacing the function of TILS using adoptive and or active and passive immunization with cytokines/cultured TILs have not proven beneficial and a possible role of local immuno-suppressors has been suggested. It has been observed that histamine, which is present in high concentration in tumor tissues, can inhibit lymphocyte migration[24],[25] and reduce the lytic ability of cytotoxic T-lymphocytes.[3] It also inhibits the natural killer cell activity.[26],[27] These actions are mediated by H2-receptors[3],[28] and therefore potentially reversible by H2-receptor antagonists.[3],[9],[28] It has also been postulated that H2-receptor antagonists can act by routes alternative to modification of TILs in cancers.[29],[30] Most studies suggest that cimetidine may improve the outcome in cancer patients by a three-pronged mechanism involving: (1) inhibition of cancer cell proliferation, (2) stimulation of the lymphocyte activity by inhibition of T-cell suppressor function, and (3) inhibition of histamine′s activity as a growth factor in tumours.[31] The projected immunostimulatory effect of H2-antagonists has been demonstrated in experimental and clinical studies done in gastric and colorectal cancer. [9],[10],[11],[12],[32],[33],[34],[35] Preoperative short-course cimetidine has been shown to affect TILs in colonic cancers and also improve survival.[6],[9],[10],[11] Although some authors have reported a survival benefit with the use of cimetidine in patients with other cancers,[12] observations to the contrary exist. [36],[37],[38] H2-receptors are present in high concentrations in malignant as opposed to benign breast tumors,[39] however, the prognostic implications of TILs, as well as the role of histamine receptor antagonists, in human breast cancers is as yet unclear on account of few published studies having addressed the issue with no definite conclusion.[7],[8],[40],[41],[42],[43] We have observed that a preoperative short course of famotidine was effective in inducing TILs in breast cancers as evident from the relative proportion of tumors demonstrating TILs in patients who received the drug, which was significantly higher than controls. Also famotidine was an important predictor of TILs in regression analysis. Earlier studies using preoperative cimetidine in breast cancer patients found no relationship between the drug administration and TILs, tumor proliferation, tissue histamine or mast cell counts.[42],[43] However, different H2-receptor antagonists have been demonstrated to have varying effects in different tumor models.[44],[45] Our present findings further strengthen our preliminary observations that famotidine induces TILs in breast cancer patients.[17] Age nodal status, menopausal status, tumor diameter, histologic type, and proliferation markers are other variables that have been thought to influence TILs in breast cancers and were therefore included in the analysis.[7],[18],[41],[46],[47] In our study however these factors were not found to be predictive of TILs. The only factor found to influence TILs was famotidine and the odds ratio for famotidine in prediction of TILs when adjusted for the above parameters was [7.324 (1.693-31.686), P = 0.008]. Although typing of TILs was possible in only some patients, when present these TILs largely constituted of subpopulation of T cells both in cases as well as controls. Our observations corroborate with evidence in existing literature, where tumor-infiltrating lymphocytes has been shown to be predominantly of T-cell types.[18] The results of our study suggest that patients demonstrating TILs in breast cancers may have improved disease-free survival (hazard ratio 3.327 91.174-9.426), P = 0.024). Even though a beneficial effect of famotidine was not evident in the initial model, it assumed borderline significance on incorporation of quadrant of involvement in the original model 3.404 (1.005-11.531, P = 0.049). Also in univariate analysis, the projected five-year disease-free survival was significantly better in patients who received famotidine as compared to controls, on comparison in patients with tumors in the outer quadrants. Quadrant of involvement is not an established prognostic factor in breast cancer, nevertheless recent studies suggest a poorer prognosis for breast cancers located in inner quadrant as compared to those situated in other quadrants. [48],[49],[50] It is possible that quadrant was a confounding factor in the analysis of the effect of famotidine on survival. Majority of the patients in our study were of the infiltrating duct carcinoma nonmedullary type and therefore a comparison amongst different histologic types was not possible. Systemic therapy in breast cancer has conventionally focused on chemotherapy and hormone therapy and the drugs used in such therapies have notable side effects. Although immune modulation therapies have been used in other cancers, it has not been adequately studied in treatment of breast cancer. The findings highlighted in the present study of the possiblitiy of immunomodulation using famotidine, a commonly prescribed drug with little adverse toxicity, may have pertinent implications in this regard. A longer follow-up to evaluate the impact on overall survival, optimum dosage, and duration of famotidine as also its relation to various other prognostic factors are the issues that need further evaluation. A double blind placebo controlled randomized trial involving larger number of patients has been designed and is underway in our Department to substantiate the findings of this study. Summary of key findings References
Copyright 2005 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn05033t1.jpg] |
| |||||||||

{kind=link}