 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
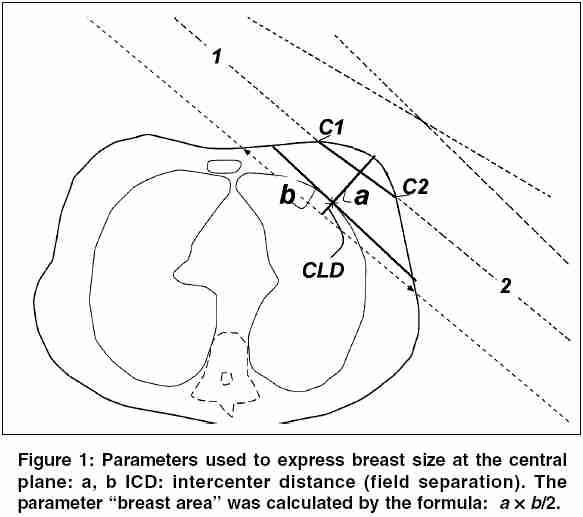
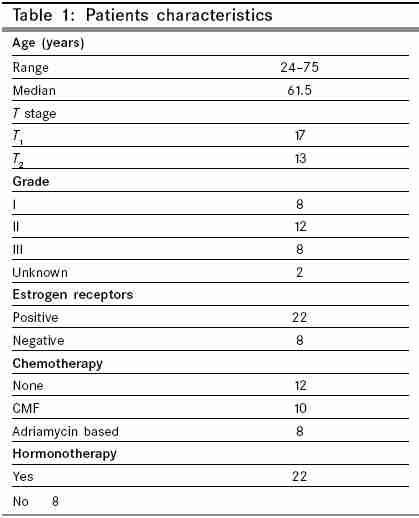
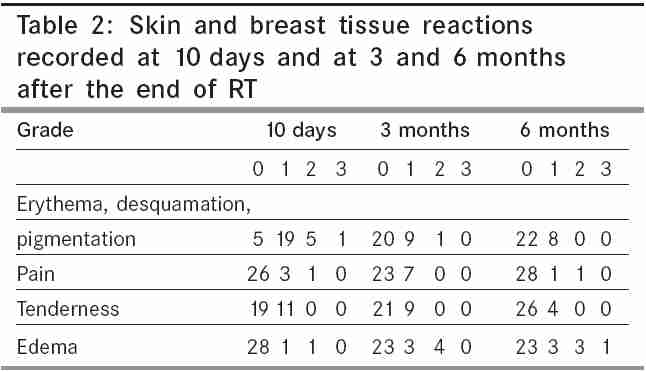
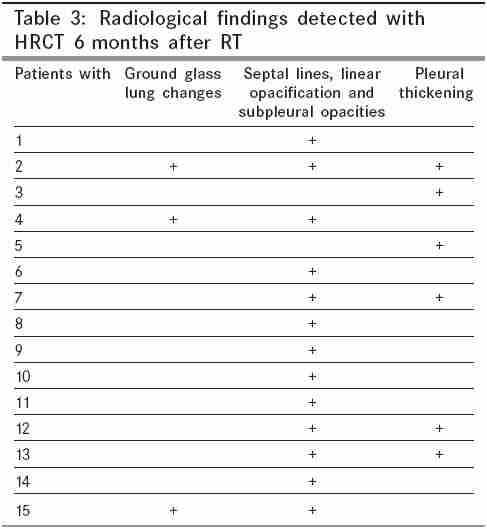
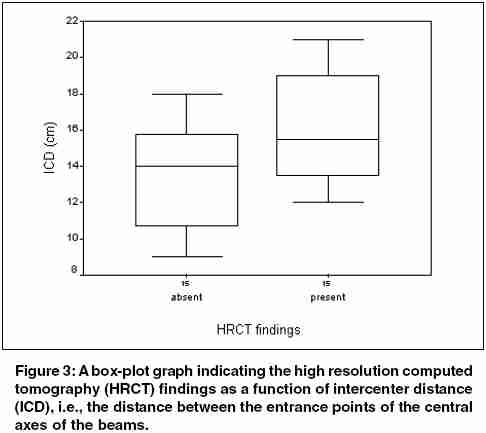
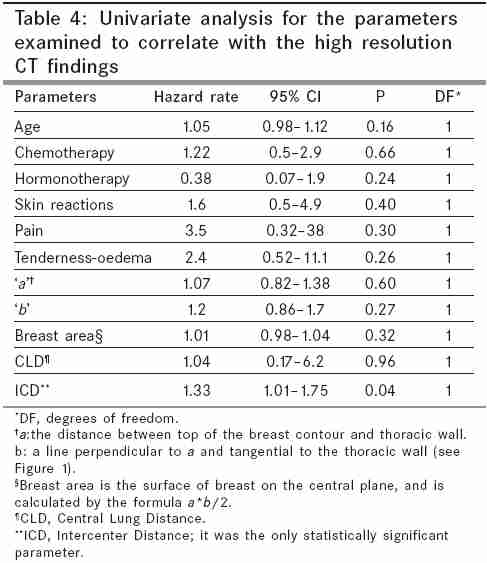
Indian Journal of Cancer, Vol. 42, No. 4, October-December, 2005, pp. 191-196 Original Article High resolution computed tomography findings on the lung of early breast-cancer patients treated by postoperative breast irradiation with a hypofractionated radiotherapy schedule Plataniotis GA, Theofanopoulou ME, Sotiriadou K, Vlychou M,1 Fountoulis GA,1 Fezoulidis J1 Departments of Radiation Oncology and Diagnostic Radiology, University of Thessalia, Greece Code Number: cn05034 Abstract Background: Hypofractionated breast radiotherapy (RT), although convenient for patients and health care systems, could have a negative impact on normal tissues such as lung. Keywords: breast cancer; high resolution computed tomography; hypofractionation; lung changes; radiotherapy Although postoperative radiotherapy (RT) for early breast cancer treated by lumpectomy is an established treatment, the issue of optimal RT fractionation schedule remains unresolved. The most widely employed schedule for whole breast irradiation is 50 Gy in 25 fractions, while a variety of shorter (hypofractionated) RT schedules have also been used in clinical practice. In a recent randomized trial Whelan et al .[1] have reported equivalent results (regarding local control, survival and postradiation effects) between the standard fractionation schedule of 50 Gy in 25 fractions and a hypofractionated scheme of 42.5 Gy in 16 fractions over 22 days, for women with node-negative early breast cancer. Short RT schedules (40 Gy in 15 fractions) have been employed traditionally in UK. [2],[3],[4] Nevertheless, radiation oncologists are usually reluctant to give a dose per fraction higher than 2 Gy for breast cancer patients because of the anticipated late radiation toxicity. One of the main organs at risk, which is involved within treatment fields, is the underlying lung. Although lung changes after breast irradiation have been extensively studied [5],[6],[7],[8],[9],[10],[11] for conventionally fractionated RT, there is a lack of data regarding hypofractionated treatments. The Department of Radiation Oncology at the University of Thessalia is the only one in central Greece serving a population of over 1 000 000 people. Furthermore, most of our patients come from remote areas and they travel daily long distances to come to the RT facility. We have been applying the schedule of 42.5 Gy/16 fr. for early breast-cancer patients, since May 2003. In the present prospective study we have performed high-resolution computed tomography (HRCT) in order to investigate the impact of larger fraction size on lung parenchyma, in early breast-cancer patients treated by the above-mentioned 16-fraction treatment. We have also tried to investigate the impact of parameters such as the breast size, hormono- or chemotherapy (CHT) on the rate of lung changes after hypofractionated RT. Subjects and methods Between May 2003 and August 2004, 126 women with invasive T1 or T2, pathologically node-negative breast cancer, were treated in our department , following breast conserving surgery and axillary dissection. Patients were treated by the 16-fractions schedule except for those with the following characteristics (who were treated by the standard fractionation scheme 23-25 × 2 Gy): levels I-II axillary dissection not performed, positive or ambiguous surgical margins, tumors pT3-pT4, presence of multicentric disease, breast deemed too large to permit satisfactory radiation therapy (i.e. maximum width of breast tissue > 25 cm), and patients treated with CHT who were unable to commence RT within 8 weeks of the last dose of CHT. Patients with the indication for CHT were referred for RT during the last cycle or after the completion of CHT. The CHT regimen was left to the discretion of the referring medical oncologist. The first 30 consecutive patients (to avoid selection) treated by the 16-fractions schedule were eligible for this prospective study. Written consent was obtained from all patients. Radiotherapy Follow-up The skin and subcutaneous tissue reactions erythema/desquamation/pigmentation, pain, tenderness and edema were evaluated as end-points. They were graded on the following five-point scale: 0 = no toxicity, 1 = slight, 2 = moderate, 3 = marked, and 4 = severe. Two independent doctors did the evaluation at each follow-up visit. The condition and symptoms of skin and breast before RT were taken as baseline. Lung function parameters (e.g., FEV1 etc.) were not measured. Radiological assessment Pretreatment HRCT was used as a baseline examination for each patient. The assessment of HRCT was done considering that the postradiation radiological findings, can be categorized as follows:[10],[11] (1) ground glass opacification, (2) alveolar infiltrates, consolidation (nodular or homogeneous), (3) septal lines, linear and subpleural opacities, and (4) volume loss, as evidenced by displacement of fissures. Statistical analysis Results Patients and treatment characteristics are shown in [Table - 1]. One patient had coronary heart disease. Three of the women were light smokers and none suffered from any concomitant respiratory illness, or required medication other than tamoxifen at 20 mg daily ( n = 22). Follow-up time ranged from 8.5 to 15 months (median 12 months). One patient developed lung metastases 14 months after RT; all other patients were free of locoregional or metastatic disease during the follow-up period. Skin and breast tissue reactions at 10 days, and at 3 and 6 months after treatment are shown in [Table - 2]. One patient experienced a grade-2 breast pain at 6 months, which resolved promptly by nonsteroid anti-inflammatory drugs. Three patients had a grade-2 and one patient a grade-3 breast edema at 6 months. In the 2/4 of these patients HRCT was positive for post-RT findings. There were 15/30 (50%) patients who developed no changes, as this was documented by a HRCT scan 6 months after radiation. Postradiation changes were detected in 15/30 patients and are summarized in [Table - 3], [Figure - 2]. These lesions were evident in the ipsilateral upper lobe of the lung, which was subjacent to the radiated mammary gland. The HRCT scan is a very sensitive method in detecting such changes and in all cases they were minimal with a very limited linear distortion of lung parenchyma. There was neither evidence of out of field pneumonitis, nor lung volume loss and displacement of fissures among the patients who participated in the present study. Also, no clinical symptoms related to lung disease were recorded. The mean value for CLDs for both HRCT positive and negative was 1.3 cm (0.4 cm SD), while the mean value for ICDs for HRCT positive and negative was 16.2 cm (3.1 cm SD) and 13.7 cm (3 cm SD) respectively [Figure - 3]. There was no correlation between CLD and ICD in the present material (Pearson correlation coefficient = 0.095, P = 0.617). Radiological findings were significantly correlated only with ICD (HR: 1.33, 95% CI: 1.01-1.75, P = 0.04), indicating a relationship between field separation and dose deposition within lung parenchyma (see [Table - 4]). Discussion The 42.5/16 fr. schedule seems to be clinically equivalent to the 50 Gy/25 fr. for these selected patients.[1] Several authors [12],[13],[14] have reported values of a/b approximately equal to 4 Gy, for lung fibrosis. At the level of 70% isodose (which enters the lung parenchyma in all patients) the calculated BED values are 47.3 and 44 Gy4 for the standard (50 Gy/25 fr.) and short (42.5/16 fr.) RT schedules.[15] The result of this calculation is in accordance with the minimal changes seen in our patients. Postirradiation lung changes have been studied for conventionally fractionated schedules. [5],[6],[7],[8],[9],[10],[11] Lind et al .[7] have shown that locoregional RT is associated with a larger incidence of pulmonary side effects compared to local RT, especially if the internal mammary nodes were included in the fields of irradiation. The mean CLD in the local RT group was 14 mm. In the same study the authors reported a negative association between sequentially administered CHT and RT-induced radiological abnormalities. A significant correlation of CLD with lung changes diagnosed with HRCT was reported by Schratter-Sehn et al .[9] in a group of 55 patients treated with a Co-60 unit (FSD = 60 cm) by standard fractionation (46-50 Gy in 2 Gy/fr.). The mean CLD in patients with and without lung changes was 2.69 and 2.06 respectively ( P = 0.000). Using a 1-4 grading scale they evaluated the HRCT at 3, 6, 9 and 12 months. At 6 months 13 patients developed radiologic changes (6 grade-I, 4 grade-II, and 3 grade-IV), and at 12 months only one additional patient developed a grade-I change. The relatively high percentage of patients (25%, 14/55) with remarkable radiologic abnormalities could be explained by the use of supraclavicular/high axillary (24/55) or internal mammary (18/55) fields and the short SSD cobalt-60 unit used in this study. Lingos et al .[5] have reported an increased incidence of radiation pneumonitis when an axillary/supraclavicular field was added to the tangential fields, and have observed an increased incidence of radiation pneumonitis in patients treated with concurrent CHT. On the contrary, Ooi et al .[10] have reported that CHT did not have any influence either on the lung function or on radiological findings. In addition, Bentzen et al .[16] have reported enhanced RT-induced pulmonary fibrosis in patients being treated with concomitant tamoxifen. An association between HRCT findings and CHT or hormonotherary was not detected in the present study. Based on the published experience we have studied the radiation-induced lung abnormalities by HRCT[17] at 6 months after hypofractionated RT. Patients with no or minimal lung changes at 6 months, have a small probability of developing further changes.[10] Our minimal radiologic findings could be attributed to both the local (and not locoregional) breast irradiation and the small CLDs obtained. The positive correlation between HRCT findings and field separation (ICD) found in the present study, could be explained by the fact that the dose was calculated at the central plane, taking into account the highest dimension of the breast. Women with a higher ICD had a higher focal dose deposition along the lower edge of the tangential fields within the lung. The ICD was more predictive for parenchymal lung changes than breast dimensions. Breast dimensions are responsible for dose inhomogeneity within the breast and are predictive for cosmetic results.[18] The acute skin reactions recorded in our patients are comparable to those reported from more protracted treatments.[19] The use of short RT schedules, especially for tumors (such as breast cancer) seen very frequently on daily practice, may have important implications for both the patients and the health care systems. The use of 16-fractions (instead of 25), saves 900 treatment sessions per 100 patients (2500-1600 = 900). This corresponds to an additional number of 56 (900 : 16) patients that could be treated by the same number of fractions. This cost-effective and convenient RT schedule seems to be safe and effective for selected patients.[1] The current data suggests that it is also safe for the underlying lung. We continue to study our patient population in regard to late radiation effects such as breast fibrosis and cosmetic results. References
Copyright 2005 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn05034t3.jpg] [cn05034t1.jpg] [cn05034t2.jpg] [cn05034f1.jpg] [cn05034f3.jpg] [cn05034f2.jpg] [cn05034t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}