 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
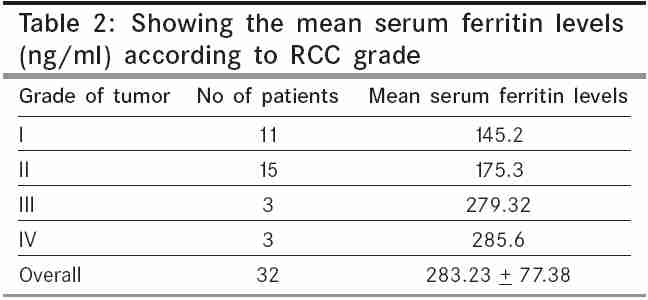
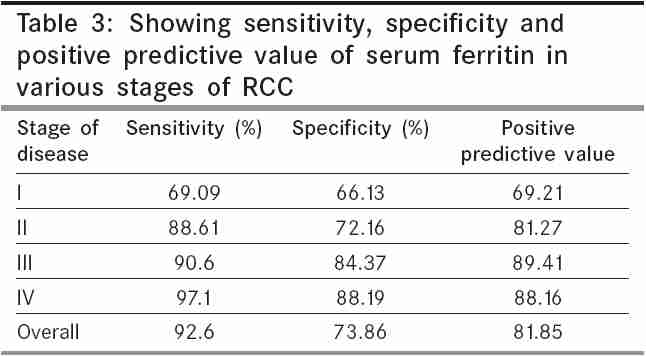
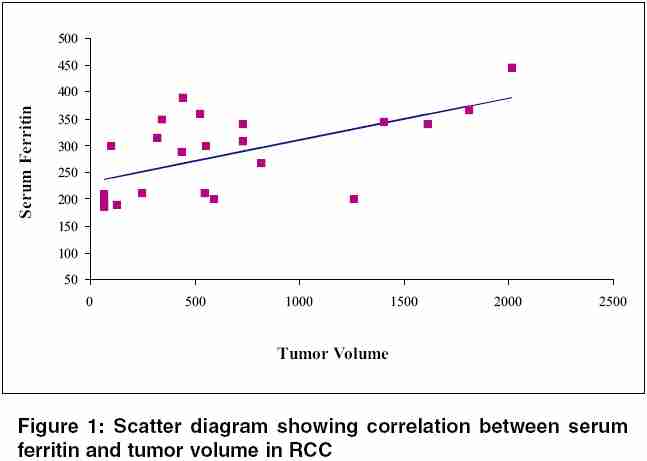
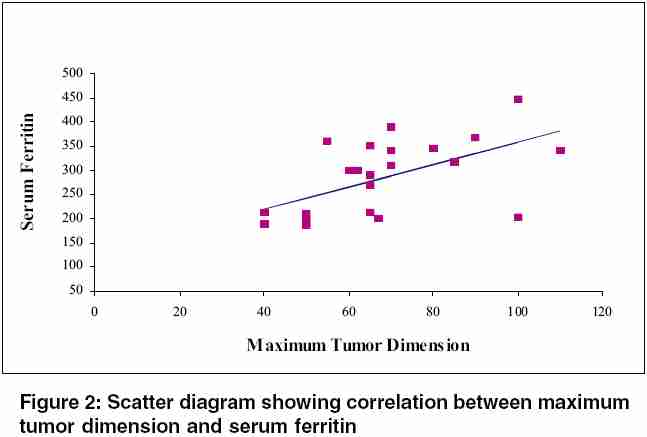
Indian Journal of Cancer, Vol. 42, No. 4, October-December, 2005, pp. 197-200 Original Article Serum ferritin in renal cell carcinoma: Effect of tumor size, volume grade, and stage Singh KamalJeet, Singh SK,1 Suri Amit, Vijjan Vivek, Goswami AK,1 Khullar M2 Department of Urology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, India, 1Department of Urology, 2Department of Experimental Medicine, Post Graduate Institute of Medical Education and Research, Chandigarh, India Code Number: cn05035 Abstract Aim: To study the levels of serum ferritin in patients of renal cell carcinoma (RCC).Patients and methods: Serum ferritin levels were measured preoperatively in 32 patients with radiological evidence of RCC using an enzyme immunoassay. The largest diameter of the primary tumor was measured in the pathological specimens in patients undergoing radical nephrectomy while in patients with nonoperable tumor maximum tumor dimension was taken from CT scan. Pathological staging was done according TNM-1997. Results: Mean serum ferritin value in patients of RCC was 283.23 ± 77.38 ng/ml while in controls the mean value was 79.98 ± 32.96 ng/ml (P < 0.001) which was statistically significant. The sensitivity, specificity, and positive predictive value of serum ferritin in RCC observed was 92.6, 73.86, and 81.85%, respectively. Conclusions: Serum ferritin levels are elevated in patients with RCC although its actual source is unclear. Further studies are needed to establish the role of ferritin in RCC. Keywords: renal cell carcinoma; serum ferritin; tumor marker Renal cell carcinoma (RCC) is the most common malignancy of kidney in the adults accounting for 3% of all cancers.[1] The RCC has been shown to secrete several hormones and biologically active substances that produce paraneoplastic syndromes or metabolic changes in the patient and some of these factors have shown to be of prognostic value. Thorough evaluation of the known prognostic factors is an essential part of the assessment of patients with RCC. This is not only critical to the planning of the therapy, but also important in predicting the outcome of the disease. Unfortunately there are no accurate tumor markers that are specific enough for either diagnosing or monitoring postoperative course of patients with RCC.[2] Several markers have shown initial promise but have proved to be of low predictive value-erythropoietin,[3] coagulation factors,[4] lipid-associated sialic acids,[5] haptoglobulins,[6] and acute phase proteins.[7] Ferritin is an iron storage protein, which is responsible for maintaining iron in nontoxic form. Much of ferretin is intracellular involved in iron storage while only a very small amount of it is present in the serum and its levels are dependent on the iron status of the body.[8] Flemming identified ferritin in 54% of tissues from RCC and showed that immunoreactive ferritin was normally present only in proximal renal tubules.[9] Recently few investigations have demonstrated increased serum ferritin levels in patients of RCC. [10],[11],[12] We prospectively studied the levels of serum ferritin levels in RCC in comparison to healthy controls. Various parameters used for comparison-tumor size, stage, grade, and volume. Materials and methods Prospectively serum ferritin levels in 32 patients of radiological proven RCC treated from October 2000 to November 2001 were analyzed. Ethical clearance for the study was obtained from the ethical committee of the institute. All patients included in the study were fully informed. Inclusion criteria, for the study was any patient with radiological evidence of RCC. Patients with liver disease, history of blood transfusion in last 6 months or anemia were excluded from the study. After taking informed consent from the patients all patients were evaluated by detail history and physical examination, hemogram, liver function tests, renal function tests, chest X-ray, and computerised tomography (CT) abdomen. Staging and grading was done according to TNM-1997 and Furhman criteria on the resected specimen, respectively. Maximum tumor dimension (in millimeters) on the resected specimen was taken as tumor size in patient undergoing radial nephrectomy, while in patients with metastasis, tumor size was obtained by adding maximum tumor dimension on CT scan abdomen and maximum dimension of metastatic lesion. Tumor volume was calculated by using formula: 4/3 × π × L × H × W [length ( L ), width ( W ), and height ( H )]. In cases of metastasis, the tumor volume was determined by sum of primary tumor volume and measurable metastatic lesion(s). The controls ( n = 32) comprised of age and sex-matched healthy volunteers. A 5-ml venous blood sample was collected in a plain vial preoperatively while sampling blood for routine workup. Collected sample was allowed to clot at 4°C and serum was obtained by centrifugation at 2000 rpm for 10 min. Serum was immediately removed and kept at -70°C until analysis. Ferritin levels in serum were estimated using enzyme immunoassay method (Omega Diagnostic Ltd., Pathozyme-Ferritin Kit, FL, USA ) which is based on sandwich technique of enzyme immunoassay using monoclonal antibodies. About 20 ml of the test sample and standard was added in the wells and 100 μl of the enzyme conjugate reagent was added and mixed for 30 min ensuring complete mixing. Then it was incubated at 20-25°C. After the end of the incubation period, the contents were discarded by turning the wells rapidly upside down over a Biohazard container and the plate was struck down several times and then against a absorbent paper. The wells were washed with water and was struck on the tissue paper once again. Then 100 μl TBM was added and was mixed for 5 s gently. Then it was incubated in dark at room temperature for 20 min. The reaction was stopped using 100 μl of the stop solution (hydrochloric acid) and mixed gently for 30 s and color change from blue to yellow was checked. The resultant color optical density was read no later than 10 min using a microplate reader with a 450-nm filter. The mean absorbance value ( A450) for each set of standard and specimen was calculated. A standard curve was prepared by the plotting the mean absorbance from each standard against its concentration in ng/ml on a graph paper. Statistical analysis Results Study comprised of 32 patients of RCC. There were 24 males and 8 females with mean age of 52.78 + 10.29 years. Neither age nor sex was found to have significant correlation with serum ferritin values. A statistical significant difference ( P < 0.001) between serum ferritin levels in patients with RCC as compared to controls 283.23 ± 77.38 ng/ml (135-445.80 ng/ml) vs 79.98 ± 32.96 ng/ml (36.2-145.1 ng/ml) was observed. On staging the tumor, there were 11, 15, 3, and 3 patients with their tumor in stages I-IV, respectively. Mean serum ferritin levels were 175.65, 217.21, 306.4, and 395.8 ng/ml in stages I-IV tumors, respectively. Mean serum ferritin levels in patients with tumor confined to Gerota′s fascia, i.e., stages I and II were 199.67 ng/ml, were significantly lower ( P = 0.031) than 326.37 ng/ml in tumor with extra gerotal spread [Table - 1]. A statistical significant difference was observed in the serum ferritin values for all stage of the tumor ( P = 0.025). Mean serum ferritin levels were 145.2, 175.3, 279.32, and 285.6 ng/ml in grade I-IV tumors, respectively [Table - 2]. There was a statistical significant difference ( P = 0.032) in serum ferritin values in grades I and II in comparison to grade IV tumors. No statistical significant difference was observed in grade I vs grade II tumors ( P = 0.76) and grade III vs IV tumor ( P = 0.86). When the highest value of serum ferritin in controls (145.1 ng/ml) was taken as a cut-off level, the sensitivity, specificity, and predictive value of serum ferritin in RCC was observed to be 92.6, 73.86, and 81.85%, respectively, as shown in [Table - 3]. Tumor volume was estimated in 26 patients on the resected specimen while in remaining eight patients volume estimation was done on CT scan. Tumor volume ranged from 65.1 to 2011.6 cm3. [Figure - 1] demonstrates the correlation between tumor volume and serum ferritin values (Pearson coefficient = 0.79, P = 0.016). The average largest tumor dimension was 6.5 + 5.3 cm ranging from 3 to 21 cm. [Figure - 2] demonstrates correlation between largest tumor dimension and serum ferritin levels (Pearson coefficient = 0.81, P < 0.001). Discussion Ferritin is a major iron storage protein in human body with liver, spleen, and bone marrow being major sites of storage.[13] Role of ferritin in various other malignancies like breast,[14] liver,[15] and hematological malignancies[16] have been investigated. Mason and Taylor were the first one to demonstrate the presence of ferritin in renal tubules using immunohistochemical staining techniques.[17] This was further demonstrated by Mufti et al . in their case report.[8] Felming et al . identified ferritin in 54% of neoplastic renal tissue using immunohistochemical staining.[9] Partin et al . reported a more intense iron staining in tumor with hemorrhage or necrosis within than in tumors which lacked these features. Based on these findings they postulated increased serum ferritin levels might represent a combination of necrotic leakage from tumor and increased hematopoietic synthesis or increased release from the tumor.[12] Other possible explanation given for raised serum ferritin levels are as an acute phase reactant, increased production or decreased clearance. Statistically significant difference in serum ferritin levels in patients of RCC in comparison to healthy control subjects observed in our study is similar to that reported by other studies in the literature.[10],[11],[12],[18],[19] We observed that as the stage, grade, size, and volume of the tumor increased, higher levels of serum ferritin levels were noted. We postulate that there are higher likelihood of having necrosis and hemorrhage in higher stage, grade, size, and volume tumor in comparison to low stage, size, grade, and volume tumors, though we did not study these two pathological factors (necrosis and hemorrhage) separately in our study. Esen et al . reported a higher serum ferritin levels with increasing stage of the disease.[18] Our results are similar to that shown by Esen et al . Partin et al . did not observe higher serum ferritin levels with increase stage of the disease.[12] Tumor size was correlated more strongly with the serum ferritin levels than the tumor volume with is different to that reported by Partin et al . who found that tumor volume to be more strongly correlating than tumor size.[12] We did not study the levels of the serum ferritin in the other renal tumors such as oncocytoma or bellini duct tumor, etc. In conclusion, our study clearly suggests that serum ferritin levels correlated well with tumor size, stage, grade, and volume. Further studies are required to establish its exact role in RCC. References
Copyright 2005 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn05035t3.jpg] [cn05035t2.jpg] [cn05035t1.jpg] [cn05035f1.jpg] [cn05035f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}