 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
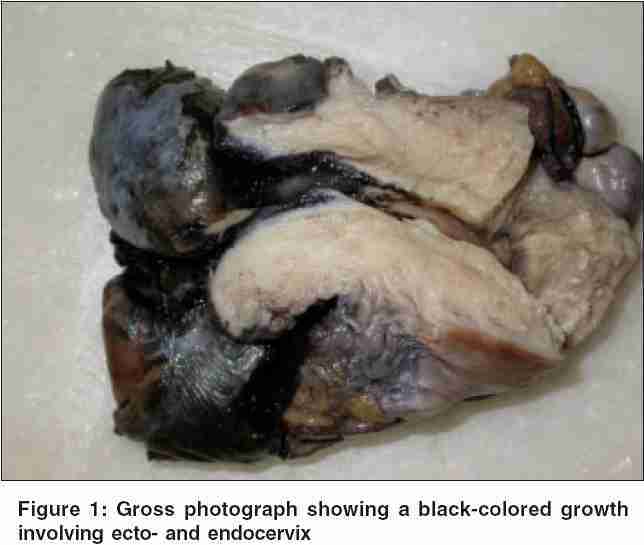
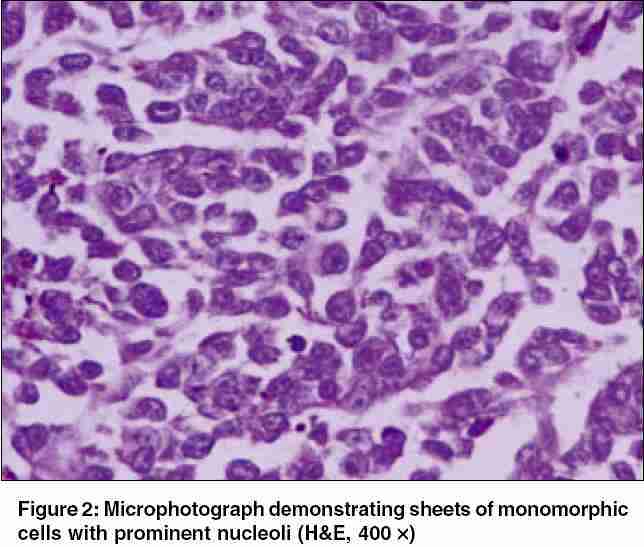
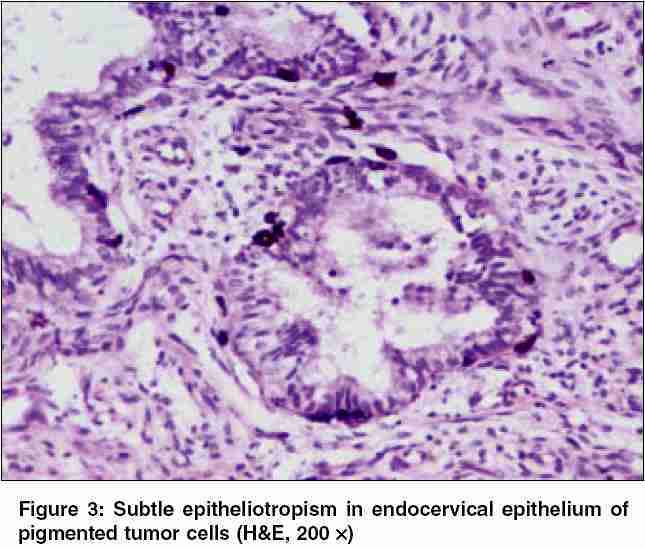
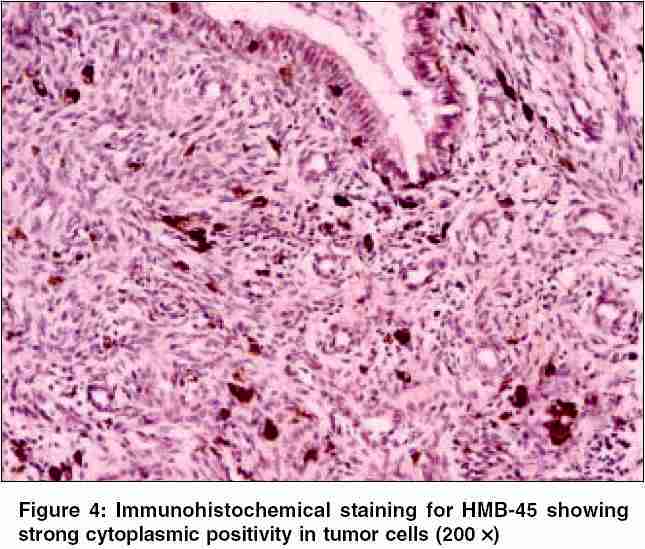
Indian Journal of Cancer, Vol. 42, No. 4, October-December, 2005, pp. 201-204 Case Reports Primary malignant melanoma of cervix - A case report Gupta R, Singh S, Mandal AK Department of Pathology, Maulana Azad Medical College, New Delhi, India Code Number: cn05036 Abstract Primary malignant melanoma is a rare neoplasm involving the uterine cervix. It may be misdiagnosed especially when amelanotic, in which case immunohistochemistry is useful in reaching the diagnosis. Though its staging and treatment are not yet well codified, prognosis is generally poor and unpredictable and hence early diagnosis is needed. We present the case of a 39-year-old female patient presenting with bleeding per vaginum. Speculum examination revealed an ulcero-proliferative growth involving the cervix. Microscopic examination of the tumor showed sheets of predominantly monomorphic cells, with few cells showing dark-brown pigment. The cells were positive for S-100 and HMB-45. In view of presence of subtle epitheliotropism, diagnosis of primary melanoma was entertained. Primary cervical melanoma should be considered while diagnosing cervical neoplasms, especially those displaying prominent eosinophilic nucleoli, even though this feature may be present only focally. Special staining and immunohistochemistry should be resorted to, whenever needed, to reach the diagnosis as early as possible. This is essential since cervical melanoma is incurable with the currently available therapies.Keywords: Cervix; immunohistochemistry; primary melanoma Primary cervical melanoma is a rare neoplasm of the female genital tract, with less than 50 cases reported in literature. Due to its often amelanotic presentation, the diagnosis may be missed or delayed. Most of the patients present in advanced stages and respond poorly to therapy.[1] Recommended therapeutic regimens for cervical melanoma include radical hysterectomy with pelvic lymph node dissection and partial vaginectomy followed by radiation therapy, either intracavitary or external beam radiation or both. However, most of the patients had poor long-term survival. Thus, early diagnosis of cervical melanoma and its differentiation from squamous cell carcinoma of cervix is essential.[1] We report clinical and histological features of a case of primary malignant melanoma of the cervix in a 39-year-old female patient. Case report A 39-year-old multiparous female presented with a history of bleeding per vaginum and abdominal pain of 2-month duration. Speculum examination showed a cervical polyp about 3 cms in diameter with congested and focally ulcerated surface. Incisional biopsy was taken and sent for histopathological examination. Microscopic sections from the biopsy showed a cellular tumor composed of small cells present in sheets. Cells had moderate amount of eosinophilic cytoplasm, predominantly monomorphic nuclei with few cells showing prominent eosinophilic nucleoli. Fair number of cells showed presence of nonrefractile dark-brown intracellular pigment. Masson′s-Fontana stain confirmed its nature to be melanin. A possibility of melanoma was suggested and the patient underwent Wertheim′s hysterectomy. We received a specimen of uterus, cervix and vaginal cuff with bilateral attached adnexae and pelvic lymph node dissection. Gross examination showed a 4 × 3 × 2 cm3 ulcero-proliferative lesion in cervix involving both ecto- and endo-cervical regions [Figure - 1]. The growth was dark on its cut-surface. Microscopic features were similar to those seen in the preoperative biopsy [Figure - 2]. Careful search and multiple sections revealed subtle epitheliotropism of malignant cells in endocervical epithelium [Figure - 3]. Tumor cells were positive for S-100 and HMB-45 [Figure - 4], thus confirming the diagnosis. Eighteen out of the 20 pelvic lymph nodes isolated, bilateral parametria and vaginal resected margins were involved by the tumor. An extensive search for a melanotic lesion in skin, uveal tract (opthalmoscopy) and other mucosal sites was negative. An abdominal ultrasound, performed preoperatively, showed normal liver, spleen, kidneys, bowel, and retroperitoneal structures. Due to the absence of a primary site of melanoma and the epitheliotropism of melanoma cells, a diagnosis of primary cervical melanoma was made. The patient received intra cavitary radiotherapy and remained disease-free for 4 months. However, she presented again with a palpable abdominal mass 4 months after initial diagnosis. A large pelvic mass encasing the left ureter and causing left hydro-ureter and hydro-nephrosis was discovered. A trucut biopsy of the mass showed recurrent melanoma. The patient was started on combination chemotherapy with dacarbazine and cisplatin. However, she died after two courses of chemotherapy without any reduction in size of the mass. Autopsy revealed widespread metastasis involving lungs, liver, and urinary bladder. Discussion Three to five percent of all primary melanoma arise from the female genital tract. Of these only about 9-13% involve the cervix, rest of them involve the vulva and vagina.[1] Thus, primary melanoma in the cervix is a rare entity. Cervical melanoma is thought to arise from the melanocytic cells of the cervix. In fact cervix is able to form the entire spectrum of melanocytic lesion known to occur ranging from benign lentigo, blue nevus to melanoma.[1] Primary malignant melanoma of the cervix has been described in a wide age range, from 19 to 83 years.[2] Vaginal bleeding or discharge is the commonest mode of presentation, similar to that seen in carcinoma cervix.[3] Melanoma in the uterine cervix may be melanotic or amelanotic and is usually composed of cells displaying variable degree of pleomorphism and prominent eosinophilic nucleoli. About half of all the mucosal melanomas are amelanotic. In the absence of pigment the diagnosis may be difficult and possibility of poorly differentiated squamous cell carcinoma, adenocarcinoma, rhabdomyosarcoma, and stromal sarcoma must be ruled out.[1] Save for the presence of pigment, stromal sarcoma was a close differential in our case. Tumor cells in our case showed only mild degree of pleomorphism. In the amelanotic variety, immunohistochemistry is helpful although, Masson′s Fontana stain may pickup small amount of pigment in cases, which appear amelanotic on HE staining. Melanoma is usually negative for cytokeratin as well as EMA and S-100 may be only focally positive.[4] HMB-45 positivity in conjunction with negativity for epithelial markers and suggestive histomorphology is specific for melanocytic lesions. Recently morphological features of primary cervical melanoma in pap smears have been published, raising the hope of early diagnosis. Cervical smear usually show scattered bizarre and pleomorphic cells containing melanin pigment.[5] Primary cervical melanoma must be differentiated from the secondary deposit from melanoma elsewhere in body. Secondary cervical melanoma may be a more ominous disease than primary cervical melanoma. Morris and Taylor have suggested the criteria for diagnosis of primary melanoma of cervix, which includes:[6]
Subtle epitheliotropism of the neoplastic cells within the cervical epithelium suggests in situ change and the possibility of primary cervical melanoma.[7] This was observed in our case also. Although Morrow and Di Siaia have suggested that a staging system based on the thickness of the primary lesion as applied in primary cutaneous melanoma is more clinically relevant, the FIGO system has also been found to correlate well with survival.[8] Primary cervical melanoma is usually discovered at an advanced stage and is no longer amenable to curative therapy. In a review of world literature of primary cervical melanoma, only three of 37 cases were Stage IA. The 5-year survival rates for stage I melanoma in this review was 25%, for stage II 14% and for stages III and IV was 0%.[7] The therapeutic recommendations for cervical melanoma include radical surgery followed by external or intra cavitary radiotherapy or both. Inspite of low level of radio-sensitivity exhibited by melanoma, irradiation is useful in palliation of an inoperable patient or as primary treatment of patient unsuitable for radical surgery.[8] Single-agent as well as combination chemotherapy using agents like melphalan, vincristine, procarbazine, and BCNU have yielded variable results with maximum effectivity seen with combination of BCNU, vincristine and DTIC (dimethyl triazeno imidazole carboxamide). However, regression, whenever achieved, has been transient.[8] Trials with immunotherapy using local bacille-calmette-guιrin or activated lymphocyte transfusion have shown promising results and may be used adjunctively following standard therapy or intermittently during prolonged therapy.[8] To conclude, primary cervical melanoma should be kept in differential diagnosis of cervical neoplasms, and the diagnosis should be confirmed using special stains and immunohistochemistry, if required. Also, melanoma of the uterine cervix is currently not curable and hence needs to be diagnosed early. References
Copyright 2005 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn05036f4.jpg] [cn05036f3.jpg] [cn05036f2.jpg] [cn05036f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}