 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
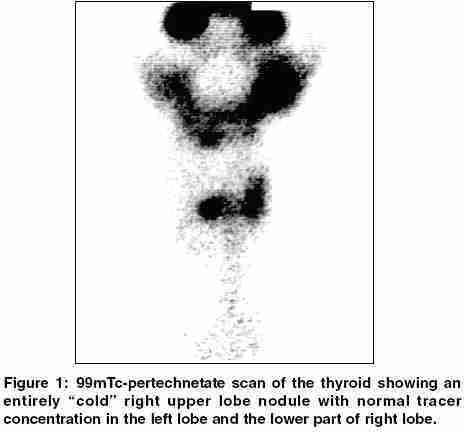
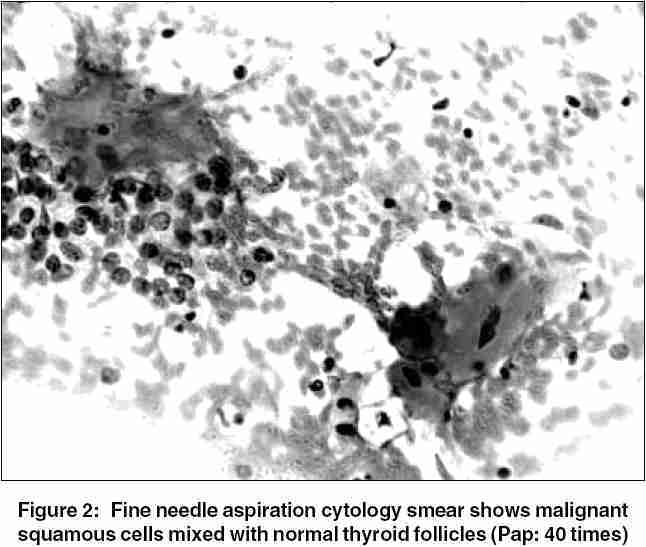
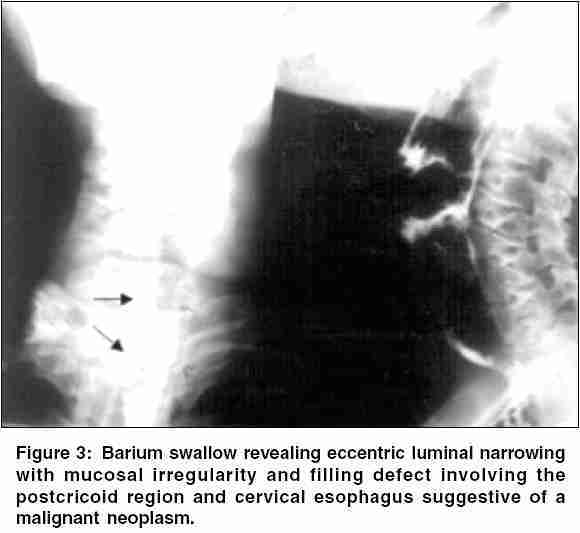
Indian Journal of Cancer, Vol. 42, No. 4, October-December, 2005, pp. 205-207 Case Reports Squamous cell carcinoma of esophagus masquerading as solitary thyroid nodule Basu S, Nair N, Borges AM* Radiation Medicine Centre, *Department of Pathology, Tata Memorial Hospital, Jerbai Wadia Road, Parel, Mumbai 400 012, India Code Number: cn05037 Abstract Secondary neoplasm of the thyroid mimicking a primary thyroid lesion is a rare finding, especially in an individual without a past history of malignancy. A case of squamous cell carcinoma metastatic to the thyroid (presenting as a solitary thyroid nodule), who had an unsuspected primary in the esophagus is described. Usually, multiple areas of the gland are involved in the secondary involvement of the thyroid. The clinical presentation of an apparently asymptomatic mass with neck lymphadenopathy, normal thyroid functions, and a cold nodule on 99mTcO4 - thyroid scan can often lead to a misdiagnosis as primary thyroid neoplasm. The present case underscores the fact that due importance to the subtle signs and symptoms and a high degree of suspicion, whenever the histology is unusual for a thyroid primary, is needed and the workup should include ruling out other primary malignancies.Keywords: Cold nodule, Solitary thyroid nodule, Squamous cell carcinoma of esophagus, 99mTcO4 - Scan of thyroid Despite being second only to the adrenal glands in terms of relative vascular perfusion, the thyroid gland is an unusual site of metastatic disease. Carcinomas metastatic to the thyroid represent a rare cause of clinically significant thyroid disease, with renal cell carcinoma (RCC) comprising 50% of the cases.[1] The diagnosis of metastatic disease should be suspected in patients with even a remote history of cancer, especially RCC, and a fine needle aspiration cytology (FNAC) revealing clear cell or spindle cell carcinoma. We herein present the clinical, laboratory, radiologic and FNAC findings in a patient presenting with solitary nodular goitre and review the related literature. Unexpected dysphagia, restricted mobility with cervical lymphadenopathies and the fact that the epidermoidal carcinoma represents an ingrown minority (0.3-0.74%) among the thyroid neoplasms, prompted us to rule out a nonthyroidal primary malignancy metastatic to the thyroid gland. Case Report A 55-year-old female from a remote village in India presented with complaints of neck swelling noticed around 6 months before which increased in size in the last couple of months. The patient also complained of mild difficulty of deglutition since last 15 days. The patient did not have any symptoms of hypothyroidism or hyperthyroidism or compressive respiratory symptoms. She had a 6 × 4 cm2 firm to hard nodule involving the right lobe and no enlargement of the left lobe. The mobility of the nodule was restricted. Multiple lymph nodes were also palpable on right side at levels III and IV. The 99mTc-pertechnetate scan of the thyroid revealed an entirely "cold" right lobe nodular goitre with normal tracer concentration in the left lobe and the lower part of right lobe [Figure - 1]. Fine needle aspiration cytology smear showed metastatic keratinising squamous cell carcinoma (SCC) [Figure - 2] and suggested to investigate hypopharynx for a possible primary. Her thyroid function test was within normal limits. Taking into consideration the complaint of recent onset difficulty in deglutition and the FNAC report a barium swallow examination and an ultrasound examination was advised. The pharyngoesophagogram [Figure - 3]A, B demonstrated evidence of eccentric luminal narrowing with mucosal irregularity and filling defect involving the post cricoid region and cervical esophagus suugestive of a malignant neoplasm. An ultrasound examination of the neck (not shown in the figure) revealed a large hypoechoic mass in lower neck posterior to right lobe displacing it anteriorly and infiltrating the right lobe from the posterolateral aspect. It showed irregular, linear echogenic area in it suggestive of air in the lumen. The mass also seemed to infiltrate the thyroid and tracheal cartilage with intralaryngeal extension. There was also a subcentimeter sized hypoechoic nodule measuring 7 × 6 mm2 involving the isthmus. Multiple rounded metastatic lymph nodes were also seen in right levels III and IV region. A diagnosis of metastatic keratinising of SCC from the cervical esophagus-giving rise to the right-sided nodular goitre was made. This was subsequently proven after surgical excision by histopathology of the thyroid and the esophagus as well as the neck lymphadenopathy. The case illustrates the often overlooked fact that thyroid can be infrequently the site of metastatic involvement. Awareness of this situation cannot be overemphasized nor can be the value of meticulous history taking and clinical examination.Discussion Primary SCC of the thyroid is an extremely rare entity. Squamous cell carcinoma arising directly from the thyroid tends to affect older patients (5th-6th decade), that have a long-standing history of goitre.[2],[3] Its etiology is unknown, the theories put forward include the "metaplasia theory" (squamous metaplasia of underlying thyroid disease) and "embryonic-rest theory" (squamous cells originating from remnant ultimobranchial duct or thyroglossal duct). Incidence is commoner in abnormal thyroids. It resembles the same of other organs varying from well to poorly differentiated lesions, with or without karatinization. The usual presenting feature is sudden increase in size of a chronic neck mass, with or without cervical adenopathy. Other accompaniments include dysphagia, dyspnea and hoarseness secondary to infiltration of adjacent structures. The tumours are usually locally advanced at diagnosis with invasion into the trachea, esophagus and major vessels. If possible, surgical resection should be attempted, followed by adjuvant radiation therapy. Clinicopathologically they share the features of anaplastic carcinoma of thyroid and prognosis also seem to be similar. They are usually radioresistant and often rapidly fatal. There have been a few cases where complete excision and postoperative radiation have been curative. Overall the median survival is of <6 months in the majority. Death is usually secondary to progression of local disease. Metastatic SCC of the thyroid is commoner. Most of the series[4],[5] report carcinoma of kidney and colon and melanoma as the frequent primaries to metastasise to thyroid. In the setting of SCC of thyroid either metastatic spread or squamous variant of undifferentiated thyroid carcinoma should be taken into account.[2] The differential diagnosis also includes tumours showing thymic or related branchial pouch differentiation, which usually occur in the neck in close relation to or within the thyroid and exhibit squamous or mucinous differentiation and have been recently designated as Spindle Epithelial Tumour with Thymus l ike Differentiation (SETTLE) or carcinoma showing thymus-like differentiation (CASTLE). Synchronous or metachronous carcinoma of the esophagus and the thyroid gland, though an extreme rarity, has been reported as solitary case reports in the literature. The thyroid carcinoma in these cases is usually of papillary or follicular type, i.e., differentiated thyroid carcinoma.[7],[8] Metastases need to be strongly considered whenever the histology is unusual for a thyroid primary. The metastatic spread to the thyroid can occur by direct extension of adjacent primaries, haematogenously or rarely by retrograde extension by lymphatic route. The etiopathogenesis of metastatic SCC of thyroid can be divided into three groups: (i) Direct extension: usually from adjacent primaries, for example, Laryngeal or esophageal carcinoma, (ii) hematogenous metastases: from lung or other primary sites, and (iii) retrograde lymphatic spread (rare). Often, multiple areas of the gland are involved. Rarely they can present as solitary nodule as seen in our case. References
Copyright 2005 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn05037f3.jpg] [cn05037f1.jpg] [cn05037f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}