 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
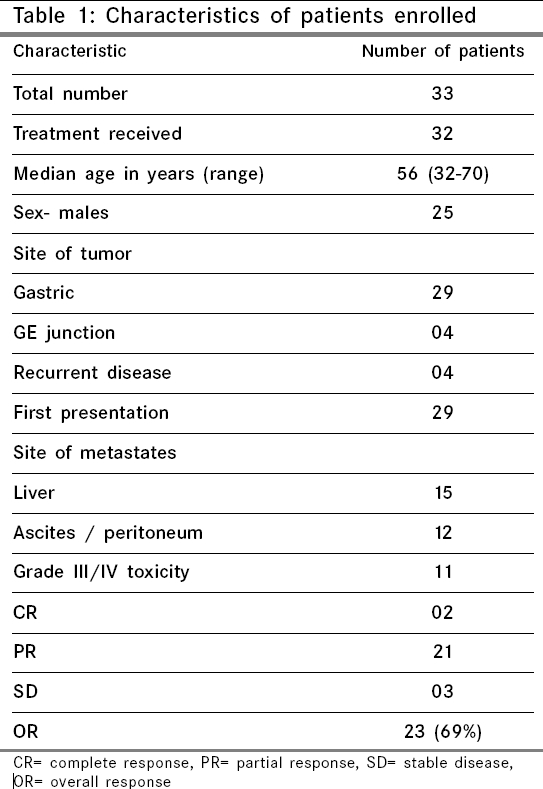
Indian Journal of Cancer, Vol. 43, No. 1, January-March, 2006, pp. 16-19 Original Article Phase II study of cisplatin, etoposide and paclitaxel in locally advanced or metastatic adenocarcinoma of gastric/gastroesophageal junction Sharma Atul, Raina V, Lokeshwar N, Deo SVS, Shukla NK, Mohanti BK Department of Medical Oncology, Institute Rotary Cancer Hospital, All India Institute of Medical Sciences, New Delhi Code Number: cn06003 Abstract Background: Unresectable and metastatic gastric cancers carry a poor and dismal prognosis. Several phase II studies have identified effective anticancer drugs.Aims: To evaluate safety and efficacy of low-dose cisplatin, etoposide and paclitaxel (CEP) based combination chemotherapy in locally advanced or metastatic adenocarcinoma of gastric/gastroesophageal junction. Setting and design:Prospective single-arm phase II study. Materials and Methods: Thirty-three patients were enrolled onto this study, out of which, all but one received cisplatin 15 mg/m 2, etoposide 40 mg/m 2 and paclitaxel 50 mg/m 2, given on day 1 and 4 every week for three weeks in a 28-day cycle. Survival analysis was done using SPSS program. Results: Median age of group was 56 years. Twenty-five were males. Twenty-nine had metastatic/inoperable disease and four patients had recurrent disease. Liver was the commonest metastatic site seen in 15 patients. With a median of 2 cycles per patient, a total of 76 cycles was administered. Grade III or IV toxicity were seen in 11 (35%) patients; diarrhea, 5 patients; vomiting, 3 patients; and neutropenia, 7 patients, 5 of whom also had fever). One patient died of neutropenic fever. Best responses, seen in 32 evaluable patients, were 2 CR (6.1%), 21 PR (63%) and 3 SD (9.2%). Four patients were considered operable after chemotherapy. With median follow-up of 11 months in surviving patients, median OS was 10 months and PFS was 8 months. Median OS was 13 months in responders versus 8 months in nonresponders ( P =0.04). Seven patients survived >12 months . Conclusion:Combination of low-dose CEP shows good clinical response and an acceptable toxicity profile in advanced or metastatic adenocarcinoma of gastric/gastroesophageal cancers. Whether addition of 5 FU or capecitabine adds to the benefit should be explored. This may be tested with other standard/conventional protocols in a randomized fashion. Keywords: Cisplatin, etoposide, gastric, gastroesophageal, paclitaxel. Carcinoma of stomach is one of the leading causes of cancer-related mortality. Screening has helped in bringing down gastric cancer-related mortality by early detection and aggressive surgery in Japan, but elsewhere, about two-thirds of patients present in advanced unresectable stage, where cure is unlikely. These patients are managed with palliative chemotherapy, radiotherapy and/or surgery. Median survival of these patients ranges from 5-7 months. Adenocarcinomas of lower one-third of esophagus and gastroesophageal junction behave like that of gastric cancer. Chemotherapy with or without radiotherapy, though used in adjuvant setting, is also used in advanced/ metastatic cancers.[1] The most commonly used agents are 5 fluorouracil, mitomycin, doxorubicin, etoposide, cisplatin and taxanes either alone or in various combinations. Response rates vary from 21 to 53% with different combinations and permutations. Various single-arm studies have shown median survival of 3.5 to 11 months.[2],[3],[4] Reported response rate with combination of DDP and VP-16 is 18%.[5] In randomized trials, DDP, 5 FU and PELF (cisplatin, epirubicin, 5 FU, folinic acid) have been demonstrated to be more effective than FAM.[6],[7],[8] Despite high responses, median survival has been below 10 months. Paclitaxel is an effective agent in esophageal and GE junction tumors.[9] Based upon activity of DDP (P), VP-16 (E) and paclitaxel (T), a combination of these drugs (TPE/CEP) was developed and tried by Lokich et al[10] with almost 100% responses in locally advanced esophageal and GE junction tumors. Based on encouraging results from this phase II study, we decided to use this combination in unresectable/metastatic adenocarcinoma of GE junction and stomach at our center; and with this, we also intended to evaluate response rates and survival. Materials and Methods This was a prospective single-arm phase II study. Study period was from May 2000 to February 2004. Inclusion and exclusion criteria Treatment regimen Response and toxicity criteria Statistical analysis Results Demographic features of 33 patients enrolled onto this study are shown in [Table - 1]. Median age was 56 years (range 32-70 years). Twenty-five were males. All patients had ′pain′ as one of the presenting symptoms; along with this, 8 patients (25%) had gastric outlet obstruction. ECOG performance status was IV in 4 patients, III in 25 patients and II in 4 patients. Twenty-nine (90%) patients had metastatic or inoperable stage at the time of presentation, whereas there was recurrence in 4 patients after initial surgery. Twenty-two patients had more than one metastatic site. Commonest metastatic sites, as expected, were liver and ascites, seen in 15 (46%) and 12 (40%) patients respectively. Even though patients were planned for 3 or 4 cycles, a total of 76 cycles only could be delivered with a median of 2 cycles (range 1-4). Many patients could not continue chemotherapy beyond 2 cycles because of economic reasons rather than toxicity or ineffectiveness. Response evaluation Survival Toxicity Discussion Advanced and unresectable gastric or GE junction cancers carry poor prognosis. Many chemotherapeutic agents have been shown to have antitumor activity; however, median survival does not exceed 5-7 months in most of the reports. Cisplatin, paclitaxel and etoposide possess antitumor activity in these tumors. Many newer agents like irinotecan, capecitabine, docetaxel and oxaliplatin also possess anticancer activity in gastric cancer. The combination of CEP used in this phase II trial is similar to the one used by Lokich.[10] 5 FU and anthracyclins have been other agents commonly used in these settings. Popular regimen of FAM has been compared with FAMTX with response rates of 9 and 41% respectively.[7] In another trial, ECF (epirubicin, cispaltin and 5FU) has demonstrated superior response rates as compared to FAMTX (5 FU, methotrexate and doxorubicin). The response rates were 45 and 21% respectively, which is equivalent to this phase II study.[11] Even though the number of patients is small in the current series, it is noteworthy that all the patients who received the therapy experienced symptomatic improvement after first cycle itself. This multifractionated protocol is aggressive in the sense that close to 20% patients had grade III or IV neutropenia. This hematological toxicity was manageable and only one required growth factor; this is despite the fact that about 90% patients had ECOG performance status of III or IV. In this trial, we could not duplicate the response rates of more than 90%, as reported in the previous study.[10] One possible reason is that median number of cycles in our study was 2 as compared to 4 in the original study by Lokich et al. Another notable difference in our study and the previous study[10] was that only 5 of our patients could be considered for further therapy (surgery or RT) as compared to 19 out of 25 patients in the study by Lokich. Again, the explanation may be, because of less number of cycles, there were not adequate responses. However, it is to be remembered that as compared to locally advanced patients in earlier series, 90% of our patients had metastatic disease, which was a clearly inoperable situation. The median survival of 10 months in our series is largely attributable to chemotherapy alone. Survival of 12.5 months was reported by Lokich et al, but it is to be remembered that about 80% of patients in their series also received local consolidation, which must have contributed to survival. We have demonstrated that patients whose disease has responded to chemotherapy had median survival of 13 months as compared to 8 months in nonresponders ( P =0.04). We hypothesize that if we can increase these responses by addition of another agent like 5 FU, which is known to have significant activity in gastric cancers or capecitabine, we should be able to increase the survival. In one of the recent phase III studies, DCF (docetaxel, cispaltin and 5 FU) has been compared with cisplatin and 5 FU. The response rates (39% vs 23%) and overall survival (10.2 months vs 8.5%) were significantly higher in DCF arm, thereby confirming the role of taxane.[12] There is a need to test this combination of CPE after adding oral capecitabine or 5 FU to other standard protocols of EAP (cisplatin, doxorubicin, etoposide), ECF or one of the 5FU-containing combinations. It is possible that with the use of new combinations, responses as well as survival may be better; in other words, what we see today for advanced colorectal cancer may be true for gastric cancers tomorrow. Conclusion Poor survival of advanced unresectable cancer of stomach/GE junction has led to initiation of various clinical trials using different chemotherapeutic drugs in different combinations. This 3-drug combination of CEP is safe, effective and well tolerated. It is possible that by increasing responses, survival will also increase. This combination warrants further studies in combination with 5 FU or capecitabine in randomized fashion.References
Copyright 2006 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn06003t1.jpg] [cn06003t2.jpg] [cn06003f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}