 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
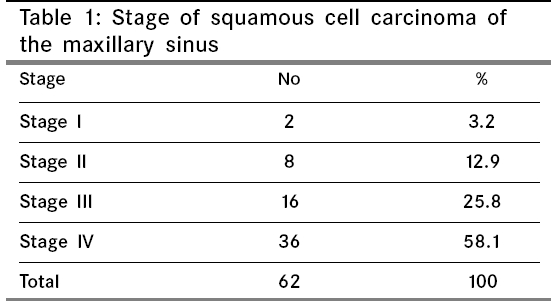
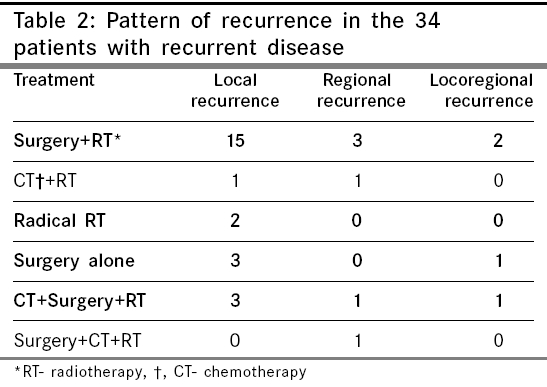
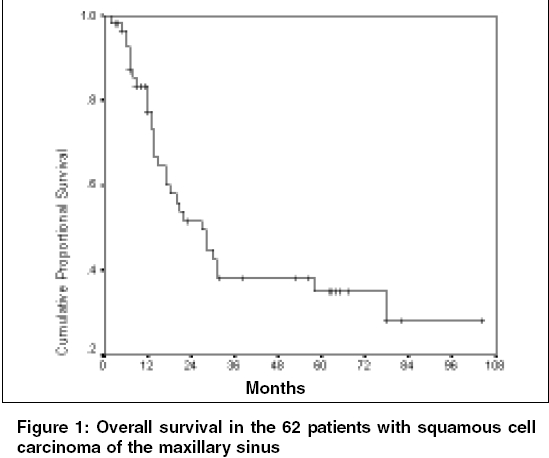
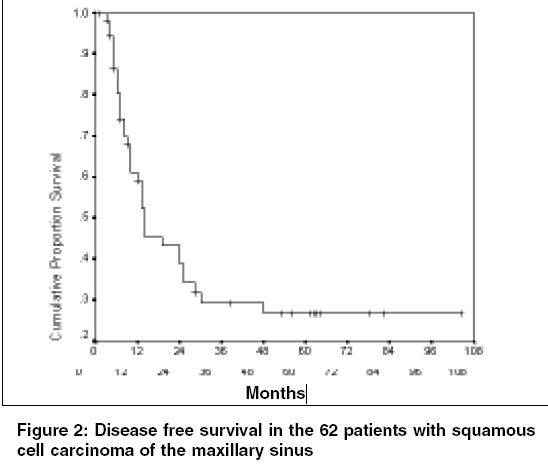
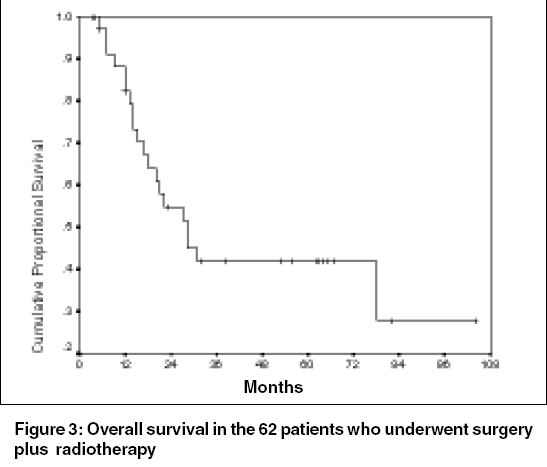
Indian Journal of Cancer, Vol. 43, No. 1, January-March, 2006, pp. 26-29 Original Article Squamous cell carcinoma of the maxillary sinus: A Tata Memorial Hospital experience Qureshi Sajid S, Chaukar Devendra A, Talole Sanjay D*, Dcruz Anil K Departments of Head and Neck Services and *Biostatistics, Tata Memorial Hospital, Parel, Mumbai - 400012, India Code Number: cn06005 Abstract Background: The optimal treatment of maxillary sinus carcinoma remains to be defined and there is a paucity of Indian studies on the subject.Aims: To present experience of management of squamous cell carcinoma of the maxillary sinus treated with curative intent at a single institution. Settings and Design:Retrospective study of patients with squamous cell carcinoma of the maxillary sinus who presented between 1994 to 1999. Materials and Methods:The records of 73 patients with squamous cell carcinoma of the maxillary sinus were analyzed. Sixty-two patients were evaluable. Forty patients (65%) were treated with surgery followed by postoperative radiotherapy, five patients (8%) were treated with radiotherapy alone, five patients (8%) were treated with surgery alone; 12 patients (19%) received chemotherapy. Statistical analysis used: Statistical analysis was done using Kaplan-Meier method. Results: The majority of patients presented with locally advanced disease (52, 84%); nodal involvement was observed in five patients (8%). The most common site of recurrence was at the primary site, which was observed in 28 patients (45%) and regional failures occurred in 10 (16%). The 3 and 5-year overall survival was 38% and 35% and the disease free survival was 29% and 26% respectively. The 5-year overall survival after surgery and postoperative radiotherapy was 42%. Conclusions:The majority of patients present with advanced disease resulting in poor outcomes to conventional treatment modalities. Locoregional tumor progression remains a significant pattern of failure. New approaches such as neoadjuvant or concomitant chemoradiotherapy with aggressive surgery need to be considered and evaluated in prospective studies. Keywords: Squamous, carcinoma, maxillary sinus, surgery, radiotherapy, recurrence, results. Introduction Carcinoma of the maxillary sinus is relatively uncommon and its treatment poses several challenges to the head and neck surgeons, radiation and medical oncologists.[1],[2],[3],[4] Firstly they often present in advanced stages. Secondly the complex anatomy and the close proximity of critical structures compromise effectual surgical excision and radiation deliverance.[1],[5],[6] Thirdly substantial uncertainty surrounds fundamental aspects of treatment hence the optimal therapy remains to be defined.[7] The purpose of this paper is to present the experience in the management of patients with squamous cell carcinoma of the maxillary sinus treated with curative intent at a single institution. Materials and Methods The medical records of 73 patients with the diagnosis of squamous cell carcinoma of the maxillary sinus treated with curative intent between 1994 to 1999 were reviewed. Of the 73 patients, 11 were excluded from the present analysis since they had undergone prior treatment at the referral centre. Our retrospective analysis included the remaining 62 patients. There were 39 males and 23 females. The median age was 55 years (range 15-70 years). The most common presenting symptom was facial swelling (57.5%), followed by oral symptoms (38.4%), epistaxis (27.4%) and nasal obstruction (11%). Facial numbness, increased lacrimation was present in two patients. On physical examination, the most common findings were facial mass in 37 patients (60%), intraoral mass in 26 patients (42%), intranasal mass in six patients (10%), palpable neck mass in five patients (8%) and trismus in five patients (8%). No patient had distant metastases at the time of diagnosis, although one patient developed distant metastases at the time of death. Histopathological diagnosis of squamous cell carcinoma was confirmed by review of pathology prior to treatment. Differentiation of squamous cell carcinoma was available in 52 of 62 patients; the tumor was well differentiated in four patients, moderately differentiated in 25 patients and poorly differentiated in 23 patients. Imaging usually comprised of computed tomography. All patients were restaged retrospectively according to the 2002 American Joint Committee on Cancer Staging System for maxillary sinus tumors.[8] The clinical stage distribution is shown in [Table - 1]. The majority of patients presented with advanced stage (III and IV, 83.9%). Nodal disease at presentation was seen in five patients (8%). Two patients had N 1 and three had N 2 disease. All the 62 patients were treated with a curative intent. Forty patients (65%) were treated with surgery followed by postoperative radiotherapy. In large lesion when it was felt surgery will not achieve Ro resection, CT or RT either concurrent or as neoadjuvant was offered. Surgery consisted of 28 total maxillectomy, three partial maxillectomy with preservation of orbital floor, four radical maxillectomy with orbital exenteration, one radical maxillectomy with total ethmoidectomy via the craniofacial approach, two medial maxillectomy and two premaxillectomy. The pathological stages were 5, T2; 15, T3 and 20, T4. Negative resection margins were achieved in 25 patients (62.5%) and 15 (37.5%) had positive margins. Three patients underwent a neck dissection and two patients with nodal disease received chemotherapy (CT) and radiotherapy (RT) and had progressive disease, hence it was elected to forgo a neck dissection. Prophylactic neck dissection was not performed in patients without neck disease at presentation. Twelve patients (19%) underwent CT; five patients received induction CT, six patients underwent concurrent treatment and one patient received adjuvant therapy. Chemotherapeutic agents used were cisplatin, methotrexate, 5-flurouracil, bleomycin and ifosphamide. RT alone was offered in five patients. The median dose to the primary site for patients receiving postoperative RT was 5000 centigray (cGy); for those receiving RT alone and concomitant CT and RT it was 6000 cGy. The regional nodes were only treated in patients with neck node involvement. Three patients with T 1 and T 2 lesions were treated with surgery alone as well as two other patients who refused postoperative RT. Overall survival and disease free survival were calculated using the Kaplan-Meier method. These end points were determined from the date of diagnosis until the event of death for survival and local, regional or distant failure for disease free survival. Results Twenty-four patients (38.7%) were alive at the time of analysis; of these 21 (33.8%) had no clinical evidence of disease. Thirty-eight patients (61%) had died during the evaluation period, 32 (51%) as a result of recurrent or persistent primary tumor, six of intercurrent disease and two patients died of second primary tumor (chronic myeloid leukemia). Overall 34/62 (54.8%) developed recurrent disease. [Table - 2] The majority of recurrences were within a year of diagnosis. The most common site of recurrence was in the primary site, which was observed in 28 of 62 patients (45%). Failure in the regional lymph nodes and distant sites were observed in 10 (16%) and one (1%) patient respectively. Isolated local failure was the most common pattern of recurrence, as demonstrated in 24 of 62 patients (38.7%). Isolated neck failure was observed in six (9.6%) patients. Only eight of these recurrences could be salvaged. Patients with metastases in the cervical nodes fared adversely and died between 4 to 22 months of treatment. The 3 and 5-year overall survival of the 62 patients was 38% and 35% respectively. [Figure - 1] The 3 and 5-year disease free survival was 29% and 26%, respectively. [Figure - 2] The group of patients who underwent surgery and postoperative RT was the largest group and had a 5-year overall survival of 42%. [Figure - 3]Discussion The patient distribution in the present series was consistent with other publications; males are more commonly affected than females, most patients present with locally advanced tumors; 83% of our patients presented with T 3 or T 4 disease. The presenting signs and symptoms result from invasion of the surrounding critical structures. In a series of 110 patients, Waldron et al[7] described pain in 59%, oral symptoms in 40%, facial swelling in 38% and nasal obstruction in 35% and epistaxis in 25% of the cases. The presentation was similar in our patients with facial swelling, oral symptoms, epistaxis, nasal obstruction and intranasal mass as the most common presenting clinical features. Clinically positive cervical metastases were present in 8% of patients in the present series. This is in keeping with the 4-15% incidence of adenopathy noted in the literature.[9],[10],[11],[12],[13] The majority of literature supports the contention that surgery and RT in combination is the most significant mode of treatment of squamous cell carcinoma of the maxillary sinus because this approach has demonstrated superior outcomes. St-Pierre and Baker[4] reported on 61 patients treated with curative intent. Of the 61 patients, 10 (16%) received resection alone, 32 (53%) underwent definitive RT and 19 received surgery and postoperative RT. The results showed a trend for improved survival among patients receiving combined surgery and RT. Paulino et al[5] reported on 48 patients, 11 (23%) of whom were treated with RT and 37 (77%) underwent surgery and postoperative RT. The results showed statistically significant improvement in 5-year local control and disease-specific survival. The overall survival rate was 0% and 52% respectively for patients treated with RT alone vs. surgery and postoperative RT. Blanco et al[2] in 106 patients noted a statistically significant improvement in the disease free survival in the patients receiving combined modality treatment compared to those receiving radiation alone (35% vs 29%; P < 0.05). There seems to be a consensus that single modality treatment is not enough for T 3 -T 4 squamous cell carcinoma of the maxillary sinus. Local recurrence remains the major cause of treatment failure in this tumor.[1],[5],[6] Pattern of failure in the present series revealed that 45% of patients failed at the primary site. Isolated local failure occurred in 38.7% of the patients and was the most common pattern of recurrence. Therefore, strategies for improving local control are peremptory for the management of this disease. Tiwari et al[11] have recommended a mandibulotomy for better clearance of the infratemporal fossa. Although, long-term results are awaited, the clearance with this approach seems to be encouraging. The addition of neoadjuvant CT has been advocated for locally advanced paranasal sinus carcinoma and has been shown to be beneficial in a selected number of patients. In one series 92% disease free survival was reported at a follow-up of 55 months following neoadjuvant chemotherapy.[14] Our experience with neoadjuvant chemotherapy was limited, however, two of our patients survived for 31 and 58 months. Similarly, use of preoperative radiotherapy with concomitant intra-arterial chemotherapy has been reported with improved outcomes, but larger studies are needed to confirm these results.[1],[5],[15],[16] In this study ten of 62 patients had disease failure in the cervical lymph nodes. The role of elective neck treatment is also debatable. Some authors recommend prophylactic ipsilateral neck irradiation based on their findings of more than 25% incidence of neck failure and high risk of distant metastases and poor survival.[3],[10],[13] Other authors do not favor ipsilateral neck treatment.[7],[11] We acknowledge that this is a retrospective study with all of the potential inherent biases associated with this type of review mainly retrospective staging and nonrandomized treatment selection. But considering the lack of prospective, multi-institutional studies almost all the previous studies have also been based on retrospective studies. Although our long-term outcomes lie within the published range the high proportion of locoregional failures and low overall survival were disappointing and suggest a need for improved local treatment. Conclusion The present study indicates that the majority of our patients presented with advanced disease resulting in poor outcomes to conventional treatment modalities. Locoregional disease progression remains a significant pattern of failure. New approaches such as neoadjuvant or concomitant chemoradiotherapy with aggressive surgery need to be considered and evaluated in prospective studies.References
Copyright 2006 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn06005f3.jpg] [cn06005f2.jpg] [cn06005f1.jpg] [cn06005t2.jpg] [cn06005t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}