 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
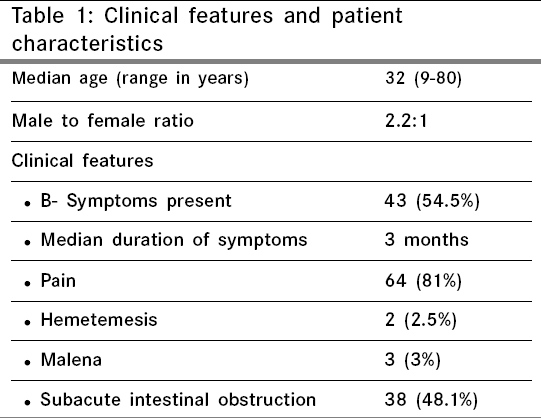
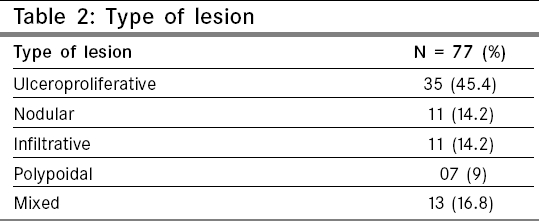
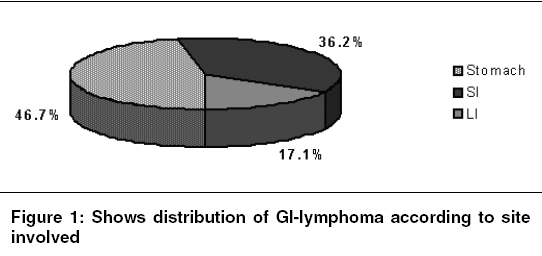
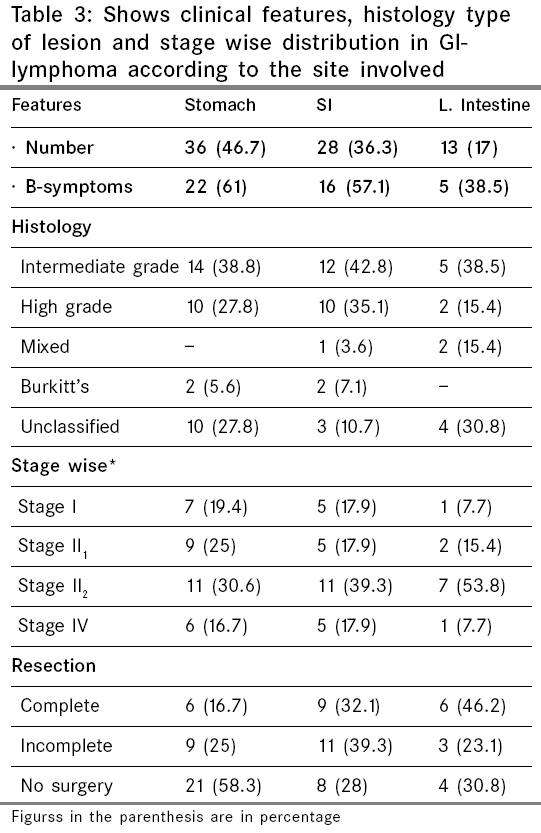
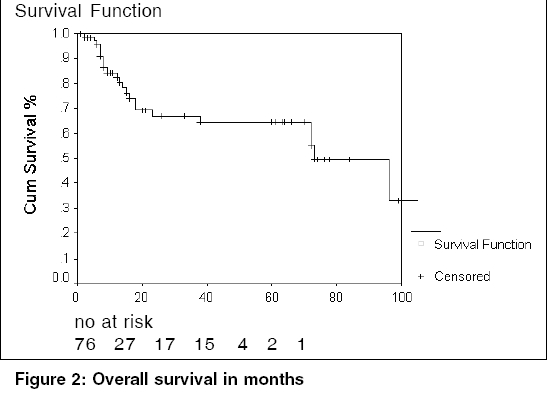
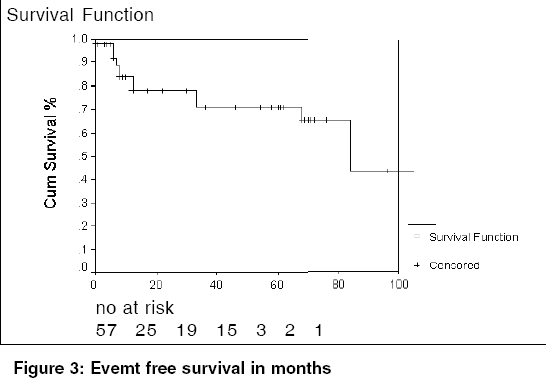
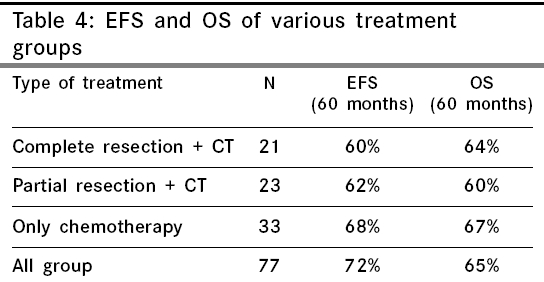
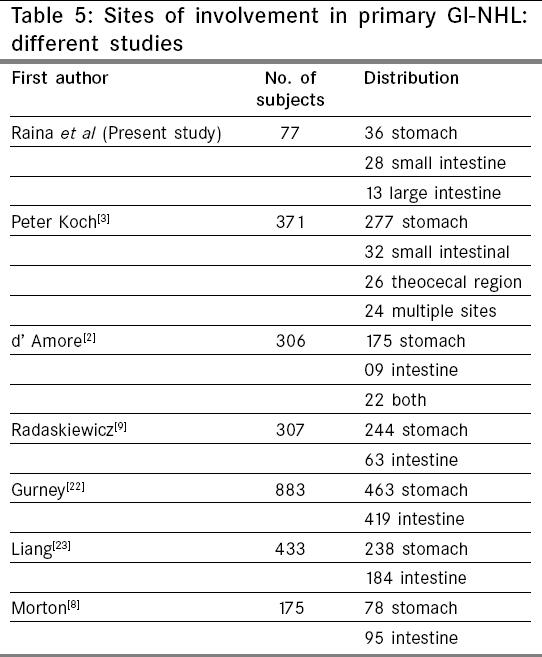
Indian Journal of Cancer, Vol. 43, No. 1, January-March, 2006, pp. 30-35 Original Article Primary gastrointestinal non Hodgkin's lymphoma chemotherapy alone an effective treatment modality: Experience from a single centre in India Raina Vinod, Sharma Atul, Vora Amish, Shukla NK*, Deo SVS*, Dawar R** Departments of Medical Oncology, *Surgical Oncology and **Pathology, Institute Rotary Cancer Hospital, All India Institute of Medical Sciences, New Delhi, India Code Number: cn06006 Abstract Background:Gastrointestinal tract (GI) is the most frequently involved extra nodal site in non-Hodgkin's lymphoma (NHL). Surgery, radiotherapy and chemotherapy (CT) have been used mostly in various combinations, but lately chemotherapy alone has emerged as an effective option. The purpose of this study is to evaluate efficacy of CT alone in treatment of primary GI-NHL and to compare the results with combined CT + surgery.Setting and design:Retrospective analysis of case records of GI NHL patients. Materials and Methods:Over a 15-year period (1986-2000), 77 new cases of primary GI-NHL were registered at our center. GI-NHL was defined according to standard criteria. All patients received chemotherapy. Results: The median age was 32 years (Range 9-80). Endoscopy / CT guided biopsies were performed in 42% (32) of patients for the purpose of diagnosis. Laparotomy was done in 58% (45) of patients to establish a diagnosis or as primary or debulking treatment. Stomach and intestines were involved in 47% (36) and 53% (41) patients respectively. Early stage disease was present in 37% (29). Seventy eight percent of tumors were intermediate to high grade, 43% (33) received only CT while 57% (44) received CT + surgery. Five years EFS and OS were: 72% and 65% for all patients; 72% and 67% for CT only group; 60% and 64% for CT + surgery group ( P =0.05). Four patients died of neutropenic infection. Conclusion: Organ-preservation strategy using chemotherapy alone (CT) can be successfully employed in a significant number of patients with primary GI-NHL. Keywords: Primary non-Hodgkin′s lymphoma of gastrointestinal tract, chemotherapy. Introduction The incidence of non-Hodgkin′s lymphoma (NHL) has been increasing over the last three decades. During the same period an increase in incidence of extra nodal NHL has also been noted.[1] Gastrointestinal tract represents the most frequent extra nodal site and it accounts for 4% of all gastrointestinal malignancies. Although many large series of primary GI-NHL describing patterns of presentation and outcome have been published the consensus over the ideal treatment for GI-NHL still remains the subject of debate.[2],[3],[4],[5],[6],[7],[8],[9],[10] Interpretation of the outcome data of these studies is hampered by differences in case selection, staging system, pathological classification and therapy. Surgery, radiotherapy (RT) and chemotherapy (CT) have all been used either alone or in combinations. Superiority of either single or combined modality over each others is still not proven. Surgery has traditionally remained the treatment of choice and chemotherapy is often used after surgery. Adjuvant radiotherapy is also practiced in some cases. Nevertheless surgery and radiotherapy are not without significant morbidity. NHL being a highly chemo sensitive disease it is now highly questionable whether radical or mutilating surgery is still necessary. Advances in endoscopic techniques for obtaining tissue diagnosis, refinements in radiological methods such as CT scans and guided biopsies and efficacy of chemotherapy have created a new option in the treatment of GI-NHL. Chemotherapy has the advantage of organ preservation; in addition it is effective for micro-metastases and hence takes care of systemic disease. In the older studies of high grade GI-NHL, chemotherapy was employed either as an adjunct to surgery or in combination with radiotherapy. However more recent studies suggests that chemotherapy alone may be as effective particularly in primary gastric lymphomas.[11],[12],[13] Materials and Methods In this study we have analyzed 77 patients of primary GI-NHL treated at our center over the last 15 years (1986-2000). This review includes clinical features, histopathological classification, site of involvement, treatment outcome and prognostic factors. Some of our patients were operated in other hospitals before being referred to us. This gave us the opportunity to compare surgery + CT vs. CT alone group. Primary GI NHL was defined according to Lewin et al i.e. patients had to present with GI symptoms or have predominant lesions in the GI tract.[14] The initial evaluation of all patients included a complete history and physical examination, complete blood count, liver and renal function tests, chest X-ray and computed tomographic scans. All patients where primary surgery was not performed underwent upper gastrointestinal endoscopic or colonoscopic studies or guided biopsies for obtaining tissue diagnosis. Bone marrow aspiration and biopsy was done in all patients. Patients were staged according to the Ann-Arbor classification as modified by Musshoff.[15] The histopathology specimens of all patients were reviewed and classified according to the International Working Formulation, which was the classification followed in our institute during study period.[16] All patients, irrespective of stage were administered chemotherapy. For patients with diffuse large B cell lymphoma and lymphoma of indeterminate histology, six cycles of CHOP (Cyclophosphamide 750 mg/m 2, doxorubicin 50 mg/m 2, Vincristine 1.4 mg/m 2 with maximum of 2 mg, prednisolone 100mg for 5 days every 21 days) were given. For Burkitt′s lymphoma, eight cycles of dose intensive MCP 842 was administered.[17] All patients who were operated outside were also given chemotherapy as above. Response criteria and end points were reported according to published guidelines.[18] Re-evaluation after completion of treatment included endoscopy, CT-scans and complete blood count and biochemistry in addition to clinical examination. Patients were examined every three months for one year and six monthly thereafter. Statistical analysis Results The clinical features and patient characteristics are given in [Table - 1 ]. Pain was the commonest symptom (81%- 64 patients); fever and weight loss were the other frequent symptoms, either of them being present in 54.5% (43) of patients. Forty eight percent of patients presented with nausea, vomiting, constipation associated with abdominal pain. Only 3% of patients presented with either hemetemesis or malena. Seventy eight percent (60) of patients had either intermediate or high grade NHL, none of our patients had low grade NHL. Four patients had Burkitt′s lymphoma. Seventeen patients (22%) could not be classified further into intermediate or high grade, as slides available were not of good quality. Stage wise, 16.8% (13) and 20.7% (16) of patients had early disease (i.e. stage I and stage II 1 respectively), while 37.6% and 15.5% had disseminated disease i.e. stage II2 and stage IV respectively. Seven (9%) patients could not be staged in the absence of the complete information. The diagnosis of lymphoma was established by endoscopy in 25(30.4%) patients, by USG/ CT guided biopsy techniques in 7 (8.9%) patients. Diagnostic laparotomy was performed in 45 (58.8%) patients. As shown in [Table - 2], ulceroproliferative type of growth was seen in (45.4%) patients. Nodular, infiltrative and polypoidal pattern was seen in 14.2% and 9% of patients respectively and mixed pattern was noted in 16.8% of patients. Stomach was the most common organ involved (46.7%-36) as shown in [Figure - 1]. Median age for small intestine NHL was much lower (30 years) compared to stomach and large intestinal NHL. B symptoms and abdominal pain was present in the majority of patients irrespective of site of involvement. There was equal distribution of patients as far as histology type of lesion and stage were concerned. Clinical features, histology, stage and site distribution has been shown in [Table - 3]. The median follow up of the cohort was 72 months (range 0 to 112 months). Main side effects of chemotherapy were myelosuppression, vomiting and diarrhoea. No patient had perforation or hemorrhage following chemotherapy. Four patients died of neutropenic fever. The OS and EFS of the patients with primary GI-NHL were 65% and 72% respectively [Figure - 2][Figure - 3]. We had three groups of patients depending on the treatment they received; 1. Surgery (complete resection) + chemotherapy, 2. Surgery (partial resection) + chemotherapy, 3. Only chemotherapy. Survival of different treatment has been shown in [Table - 4]. A total of 23 deaths were recorded during the study period. Eight patients died of disease progression after relapse, four of neutropenic infection, nine patients did not achieve CR and died, two died in CR due to causes unrelated to the disease. Patients who did not achieve CR were treated with salvage protocols like IMVP-16 (Ifosfamide, Methotrexate and VP-16) or MINE (Mitoxanterone, Ifosfamide and VP -16). Prognostic variables Discussion Primary GI-NHL represents a heterogeneous disease with regard to various characteristics like stage, site of involvement, histological subtypes and treatment offered. The commonest presenting symptom in GI-NHL is abdominal pain.[7] In our series, 81% of patients had abdominal pain as presenting feature. More than half (54.5%) of our patients had B symptoms, which is higher than Western data.[3],[19],[20],[21] We have noted equal distribution of gastric and intestinal lymphomas, Gastric: 46.7%, Intestinal 53.3%. [Table - 5] summarizes anatomic location of the initial disease in the GI tract reported in recent studies.[2],[3],[8],[9],[22],[23] In the majority of the studies, stomach is the commonest site of involvement. With the introduction of the entity MALT lymphoma by Issacson, more and more gastric MALT lymphomas are diagnosed.[24] As reported in recent series by Peter et al , 40% of stomach NHL were of MALT type.[3] In our series, there was no patient with MALT lymphoma. Fifty two percent of our patients had disseminated disease at the time of diagnosis (stage II 2 E + stage IVE) in contrast to the Western reports of 10%-31%.[7],[3] Surgery with or without chemoradiotherapy has been the mainstay in the treatment of GI-NHL but this may be questioned. In a report by Brigitte et al 90% of cases underwent surgery followed by chemotherapy with 61% OS at 2 years.[6] Two important large prospective studies have been reported recently. In German trial, of 371 patients with primary GI-NHL 44% had intermediate to high-grade lymphoma; received surgery + chemotherapy and had 5 year overall survival of 64%.[3] In a study on gastric lymphoma from Mexico 589 patients were randomized to either surgery (S) with or without radiotherapy (SRT) and chemotherapy (SCT) and chemotherapy (CT) alone, actuarial curves at 10 years showed that overall survivals (OS) were: S: 54%; SRT: 53%; SCT: 91%; CT: 96% ( P < 0.001). Late toxicity was more frequent and severe in patients who underwent surgery.[11] We believe that advanced primary GI-NHL requires a systemic rather than a local approach and therefore we administered chemotherapy in all patients. Many of our patients underwent surgery (59%) before coming to us and this gave us an opportunity to compare the results in two groups. We had 67% survival at 5 years in patients receiving only chemotherapy as compared to 60-64% in surgery + CT arm (incomplete surgery, chemotherapy and complete surgery and chemotherapy respectively), which had borderline statistical significance ( P =0.05). Presentation of GI-NHL in India is different from that in developed world. Different features of Indian studies are summarized in [Table - 6]. All the studies reported from India are retrospective and have small number of patients. Survival with surgery and RT was reported to be 44% in stomach & 24% in intestinal NHL which is lower than surgery and chemotherapy (73% for stomach and 76% for intestinal type).[25],[26] Patients in the study by Chandran et al had OS of 47% at 5 years and the treatment modalities used were surgery + RT, surgery + CT, surgery + CT + RT and CT + RT. [4] OS in our study was 60% for stomach and 69% for intestinal type at 5 years. This study questions the need for surgical intervention in diagnosis and treatment of GI-NHL except in emergency situations. There is a need to have prospective studies in this country by various centers to come out with definitive treatment guidelines. Conclusion Treatment of primary GI NHL is changing and chemotherapy alone is emerging as an attractive option. This has been brought about by: 1) advances in endoscopic diagnosis whereby a laparotomy is no longer necessary; 2) very high efficacy of chemotherapy; 3) studies showing that extensive resection may not be necessary with emphasis shifting to organ preservation and finally the concept that; 4) NHL being a systemic disease, a systemic approach like chemotherapy would be more appropriate. Our study indicates that results of chemotherapy alone are not inferior to resection with chemotherapy.References
Copyright 2006 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn06006f2.jpg] [cn06006f3.jpg] [cn06006t5.jpg] [cn06006t4.jpg] [cn06006t2.jpg] [cn06006f1.jpg] [cn06006t3.jpg] [cn06006t1.jpg] [cn06006t6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}