 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
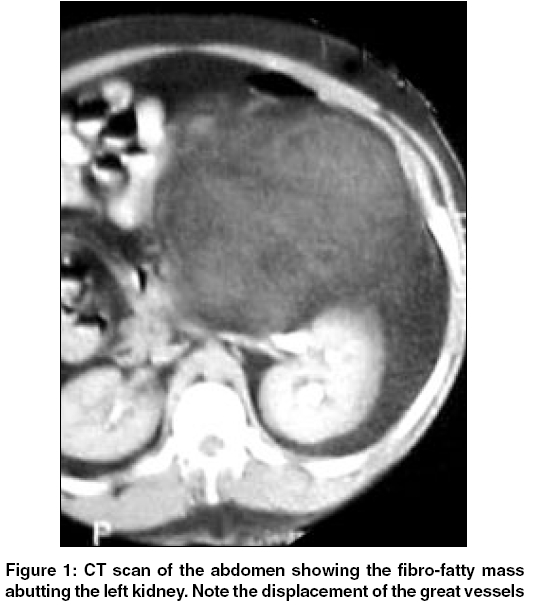
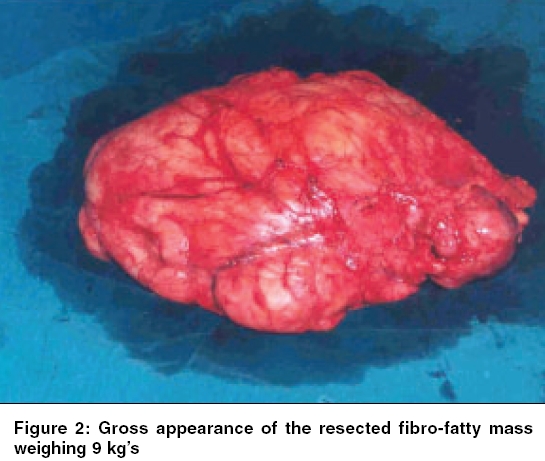
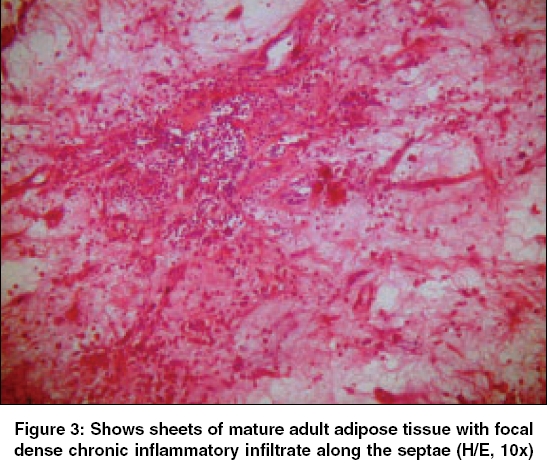
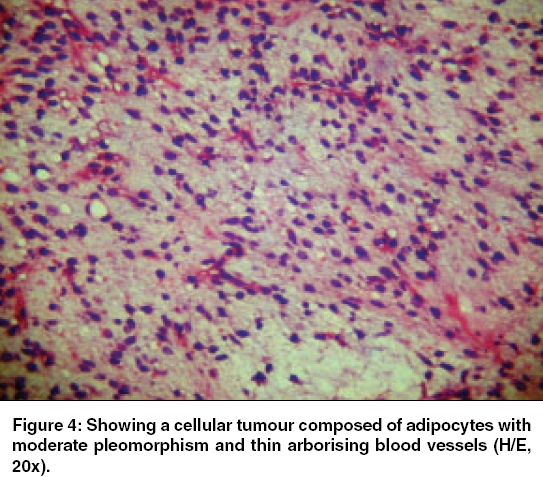
Indian Journal of Cancer, Vol. 43, No. 1, January-March, 2006, pp. 36-38 Case Report Inflammatory variant of a well-differentiated retroperitoneal liposarcoma: Case report of a rare giant variety Mehrotra PrateekK, Ramachandran CS, Goel Deep, Arora Vijay Department of General Surgery, Sir Ganga Ram Hospital, New Delhi - 110060 Code Number: cn06007 Abstract Inflammatory liposarcoma is a rare variant of a well-differentiated liposarcoma (WDLPS). We present a case of a 37 years old male who had a giant variety of this inflammatory WDLPS. CT scan revealed a large abdomino-pelvic mass abutting the left kidney and pushing the IVC, Aorta and the left ureter across the midline. CT guided FNAC did not reveal any malignant cells. A large 9-kg fibro-fatty mass, which appeared irregular, congested and bosillated was excised. Microscopic picture revealed foci of fibrosis with mature adipose tissue. Lymphocyte and plasma cell infiltrate was abundant along with multi-nucleate giant cells and few lipoblasts. There are no case reports of a giant inflammatory variant of WD-LPS in world literature and this is the first of its kind from the Indian sub-continent. We present a case report of this rare giant variant of inflammatory WDLPS and discuss the review of literature.Keywords: Retroperitoneal liposarcoma, inflammatory differentiated liposarcoma, giant liposarcoma. Introduction Well-differentiated liposarcoma (WDLPS) is a low-grade malignant mesenchymal tumor. It includes the sclerosing, spindle cell, inflammatory, adipocytic and dedifferentiated rare subtypes.[1] WDLPS is the second most common liposarcoma (LPS) after the myxoid variety. Presence of abundant inflammatory cells is uncommon in WDLPS.[2] There are only two small series of 10 cases[2] and 9 cases[3] of inflammatory WDLPS reported in literature. Giant variants of inflammatory retroperitoneal WDLPS have not been reported, though there are case reports of giant LPS containing myxoid and dedifferentiated elements.[4] Till date only one case of an inflammatory WDLPS has been reported from the Indian subcontinent.[5] This is only the 2nd case and first of its kind of a giant variety of retroperitoneal inflammatory WDLPS reported from the Indian subcontinent.Case Report A 37-year-old male presented with epigastric pain for 10 days with gradual increase in weight and abdominal girth over the past 5 years. On examination, a diffused, non-tender, non-mobile mass occupying the whole of the left side of the abdomen could be felt. The margins were ill defined. His hemogram, renal, liver functions and CEA levels were within the normal range. A contrast enhanced CT scan revealed a large fatty retroperitoneal mass abutting the left kidney causing its malrotation along the horizontal axis with the left ureter being displaced to the right of the spine in its upper 2/3rd [Figure - 1]. The Aorta and IVC were displaced towards the right and the colon was displaced anteriorly. IVP confirmed the findings. An angiogram did not reveal any obvious major arterial feeder. CT guided FNAC of the mass revealed mature adipocytes with no evidence of malignant cells. Excision of the retroperitoneal tumor was done through a trans-peritoneal approach. The large fat containing retroperitoneal abdomino-pelvic mass was abutting the left kidney and had pushed the bowel anteriorly. Mass was densely adherent to the left Gerota′s fascia. Gross appearance revealed a 35 x 28 x 13 cm irregular bossilated fibro-fatty mass weighing 9-kgs. [Figure - 2] Cut section shows homogenous yellow brown appearance. Microscopic picture revealed mature adipocytes with foci of fibrosis. Abundant inflammatory cell infiltrate of lymphocytes, plasma cells and a few polymorphs were seen. [Figure - 3] A few scattered tumor cells had pale, granular to vacuolated cytoplasm with large hyper-chromatic pleomorphic nuclei along with multi-nucleate giant cells and stray lipoblasts were present. [Figure - 4] The resected margins were free from the tumour. No radiotherapy or chemotherapy has been given in the post-operative period. The patient has been on regular follow up for the past 24 months. There has been no recurrence. Discussion Liposarcomas are commonly found in the thigh and the retro-peritoneum. Their clinical presentation of inflammatory WD-LPS is not significantly different from their commoner counterparts where no inflammatory infiltrate is seen, but at times patients may present with pyrexia of unknown origin.[5] At times the extensive lympho-plasmocytic infiltration mimics an inflammatory pseudotumour and Castlleman′s disease.[2] Key histological features encountered are nodular lympho-plasmocytic aggregates containing fibroblastic elements, frequently with plasma cell rich zone and scattered atypical, multi-nucleate cells.[2] There are reports to suggest that T cells are the prominent type[3] but workers have also suggested a predominance of B cells.[2] Retroperitoneal localization is a significant negative prognostic factor for recurrence. Other factors influencing survival rates are the tumour size, depth, invasion of surrounding structures and completeness of surgical excision. Studies have reported a recurrence rate of 27%.[6] Like most of the sarcomas, lung is the commonest site of metastasis. Other sites of metastasis are vertebra, liver and brain.[6] Radical surgery is the treatment of choice for retroperitoneal sarcomas. Our case did not have any evidence of metastasis and on surgery it was only found to be adherent to the Gerota′s fascia. The resected margins were negative. 24 months follow up has not revealed any recurrence or metastasis. There is a scarcity of reports of giant liposarcomas in world literature. The inflammatory variant of WD-LPS has been underreported in world literature with only two small series documented till date.[2],[3] There has been only one case of inflammatory WD-LPS reported from the Indian subcontinent. This is the first case of a giant retroperitoneal inflammatory WD-LPS being reported. Giant retroperitoneal LPS of the mixed type weighing 17 kg′s[7] and dedifferentiated variety weighing 18 kg′s[8] have been reported but there are no reports of a giant inflammatory WD-LPS. The tumour in our case weighed 9 kg′s, which is one of the largest reported cases of inflammatory WD-LPS of the retroperitoneum. The mean size of retroperitoneal liposarcomas′reported is 15.7 cm.[9] The tumour in our case was much larger (35 x 28 x 13 cm) than the average reported size. In conclusion, inflammatory variant of well-differentiated liposarcoma is a rare tumour found mainly in the lower limb and retroperitoneum. This is one of the largest reported cases of an inflammatory WD-LPS of the retroperitoneum. References
Copyright 2006 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn06007f2.jpg] [cn06007f4.jpg] [cn06007f1.jpg] [cn06007f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}